Download
1 / 26
300 likes | 345 Views
Carbapenem Resistant Enterobacteriaceae: The Nightmare Bacteria Comes To Newfoundland. Ashley Ryan BN RN ICP Mary Ann Head BN RN ICP Infection Prevention and Control Program Eastern Health. Objectives. Think Global Act Local The Tongue T wister Why a Nightmare Bacteria?

E N D
Carbapenem Resistant Enterobacteriaceae: • The Nightmare Bacteria Comes To Newfoundland • Ashley Ryan BN RN ICP • Mary Ann Head BN RN ICP • Infection Prevention and Control Program • Eastern Health
Objectives • Think Global Act Local • The Tongue Twister • Why a Nightmare Bacteria? • Treatment Options • History of Origin • The Numbers Don’t Lie • Cases • Moving forward: What we have learned
Think Global-Act Local • The emergence and dissemination of antimicrobial resistance is a serious threat to public health world wide • “Everything is only a plane ride away”-The world is getting smaller. People often travel for work to foreign countries more today than ever before. • Infection Control plays a key role in the prevention of transmission in health care settings through procedures and policies that are put in place. • Infection Control evolves as the world gets smaller
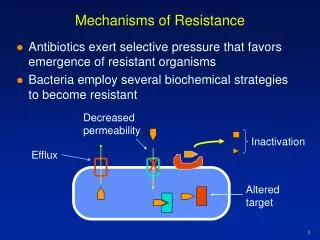
The Tongue Twister Of ARO’s:Carbapenem Resistant Enterobacteriaceae • Carbapenem Resistant Enterobacteriaceae or CRE are a family of germs that are difficult to treat because they have high levels of resistance to antibiotics. • Examples of Enterobacteriaceae are Klebsiella species and Escherichia coli (E. coli) which is a normal part of the human gut bacteria, that can become resistant to the carbapenem drug group. • Types of CRE are sometimes known as KPC (Klebsiella pneumoniae carbapenemase) and NDM (New Delhi Metallo-beta-lactamase). • Typically, Healthy people usually do not get CRE infections • Usually, CRE Infections happen to patients in hospitals, nursing homes, and other healthcare settings. Patients whose care requires devices like ventilators (breathing machines), urinary (bladder) catheters, or intravenous (vein) catheters, and patients who are taking long courses of certain antibiotics are most at risk. • CRE Bacteria are easily spread from asymptomatic carriers through direct contact with blood or bodily fluids or the environment.
CRE bacteria have become resistant to most antibiotics available to treat infections, meaning that most antibiotics will not work to fight the infection. This is where they get the name “Nightmare Bacteria” Infections of this nature are very difficult to treat, and can be CRE Bacteria can contribute to death in up to 50%of patients who become infected
Treatment Options • Carbapenems are a drug group used to treat severe infections and are high on the totem pole of antibiotics. • Carbapenems, until this resistance occurred, were the most reliable antibiotics against Klebsiella species, Escherichia coli, and other Enterobacteriaceae. • When carbapenems were discovered,nearly all Enterobacteriaceae were susceptible to carbapenems • There are very few drugs to treat bugs resistant to carbapenems. • Patients can be tested for Colistin and Teqecycline sensitivity to see if these drugs can be used for treatment • No new gram negative drugs in the pipeline
Thinking Global…..Where Did CRE Originate? • First documented case was discovered in North Carolina in 1996 and was designated K pneumoniae carbapenemase (KPC-1) • Extending globally, KPC is now endemic in the Mediterranean basin, including Israel, Greece, and Italy; in South America, especially Colombia, Argentina, and Brazil; China and USA. • OXA-48 (Oxcillinase resistant) • Discovered in New Delhi, India in 2008 -New Delhi metallo-beta-lactamase, or NDM-1 • NDM-1 has spread globally since it’s discovery in 2008 • However, multiple strains found in India and transmission is very high. Major issues in India due to poor sanitation, living conditions, and over populating. Creates a perfect environment for transmission.
The Numbers Don’t LieThe Statistical Facts: • According to CNISP 2014, the CRE infection rate is 0.22% per 10,000 days • First case in Canada was reported in Ottawa in 2008. Patient who had a travel history to the US • 2 Separate outbreaks reported in Montreal ICU which included 9 cases and 4 deaths attributed to their infection • 140 cases reported nationally of both infections and colonization's VS 5000 MRSA colonization's • To date, there are 2 CRE cases that have been identified in Newfoundland and Labrador that were acquired internationally
Acting Local… • A patient who had spent time in a healthcare facility overseas was transferred to Eastern Health • IPAC was contacted and suggested droplet and contact isolation for patients arrival. • Patient was screened for MRSA and VRE as per policy. • Public Health Lab discussions ongoing regarding CRE screening, and sample was sent to Winnipeg National Microbiology lab for testing.
Back to Basics…. • CRE was detected • Mass education completed on CRE to the patient, family and staff members involved • Back to basics-Reinforcement of IPAC principles • Donning and Doffing • Contact isolation • Equipment Dedication • Group huddles were done on the unit with nursing staff, managers, Environmental services staff • CDC and Public Health Agency were used as resources for education • Patients chart was flagged as well as in the meditech system
Case 2:Acting Local… • A Patient with recent travel history, presented to the ER with nausea and vomiting and had a complex medical history • Had full septic work up • Sample returned positive for highly resistant forms of bacteria. Was sent to National Microbiology lab in Winnipeg where it was returned positive for CRE. • Mass education completed. • Patient was deemed a good candidate for a rehabilitation program
Case 2: Acting Local… • Mass education completed with the staff regarding CRE. • Processes put in place for strict contact isolation, private room, private washroom, enhanced cleaning. • Many day to day reassessments from IPAC • Eventually, patient was able to be discharged from the inpatient unit and seen on an outpatient basis. • Further mass education and processes put in place for outpatient department • Outpatient experience was more challenging due to movement of patient, use of recreation tools for rehab and accommodating a private washroom
IPAC Detectives…. • “Detective work” completed • Practices and procedures were put in place. • Also determined the needs of this patient for the future and what practices needed to be initiated-looking ahead. • Great involvement from EVS staff.
What Have We Learned? • Routine Practices are essential! • Never assume people understand abbreviations. CRE, ARO, MRSA can mean multiple things to different groups of people. • Reinforcing basic principles of IPAC are the key to success • Identifying colonized patients is vital to limiting risk for transmission • Multidisciplinary approach including positive working relationships are essential in Infection Control. • Change in practice is positive: • New Management of ARO screening policy implemented at Eastern Health • Screening tool has changed to now include screening for CRE for both acute and long term care patient screening. • Eastern Health now has the ability to test for CRE. Resources for Information: • CDC • Public Health Agency of Canada • Guidance management document available from PHAC