Methylphenidate Transdermal Patch
Methylphenidate Transdermal Patch. Paul J. Andreason, MD Acting Deputy Director Division of Psychiatry Products Center for Drug Evaluation and Research, FDA. Methylphenidate and ADHD over time. NDA 10-187 Ritalin Tablets (methylphenidate HCl) December 5, 1955 “Minimal Brain Dysfunction”

Methylphenidate Transdermal Patch
E N D
Presentation Transcript
Methylphenidate Transdermal Patch Paul J. Andreason, MD Acting Deputy Director Division of Psychiatry Products Center for Drug Evaluation and Research, FDA
Methylphenidate and ADHD over time • NDA 10-187 Ritalin Tablets (methylphenidate HCl) December 5, 1955 “Minimal Brain Dysfunction” • 1962 Congress amended the Food Drug & Cosmetic Act to require that a drug demonstrate effectiveness prior to its approval
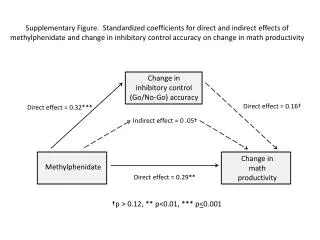
Basis for Approval • Established Diagnosis of ADHD • Improvement on Class Room Measures of Attention and Behavior in Double Blinded Randomized Placebo Controlled Trials • *Swanson, Kotkin, Agler, M-Fynn and Pelham (SKAMP) laboratory school rating scale • Inattention/Over-activity with Aggression (IOWA) Conners scale.
Formulation Changes • Extended Release • 18-029 Ritalin SR (methylphenidate HCL) Sustained-Release Tablets 3/30/1982 • 21-121 Concerta (methylphenidate HCL) Extended-Release Tablets 8/11/200021-259Metadate CD (methylphenidate HCL) Extended-Release Capsules4/3/2001 • 21-284 Ritalin LA (methylphenidate HCL) Extended-Release Capsules 6/5/2002 • 21-802 Focalin XR (dex-methylphenidate) Extended Release Capsules 5/26/ 2005
Formulation Changes • Solutions • 21-419 Methylin (methylphenidate HCL) Oral Solution 12/19/2002 • Chewable Tablets • 21-475 Methylin (methylphenidate HCL) Chewable Tablets 4/15/2003
Drug Substance Changes • Stereo-specific • 21-278 Focalin (dexmethylphenidate HCL) Tablets 11/13/2001 • 21-802 Focalin XR (dexmethylphenidate HCL) Extended Release Capsules 5/26/ 2005
Studies Consistently Positive • Studies are often positive at all measured time points • Measurable treatment effects are both statistically and clinically significant • Stimulants are a very reliable mainstay in the treatment of ADHD
Methylphenidate Patch Change in route of methylphenidate administration
Regulatory History • Initial NDA Application June 27, 2002 • Not Approved April 25, 2003 • Significantly overmedicates children at inappropriate times of the day and leads to unacceptable adverse events not associated with other once a day products available • Complete Response to the Not Approved Action Letter June 28, 2005 • Action Due-Date December 28, 2005
Clinical Issues • Efficacy achieved at expense of excess drug exposure and unacceptable incidence of adverse events • insomnia, anorexia, and significant weight loss in the short-term. • These adverse events would be expected to result in possible growth retardation or other serious adverse consequences with more chronic treatment. • Other products approved for once a day dosing in this population are not associated with this level of exposure • Patients might benefit from decreasing the wear-time of the patch
d-MPH Cmax for Concerta and MTS in the Phase III Clinical Study
Therapeutic Effect Drug-induced improvement in sustained attention is entirely attributable to the d-enantiomer • Srinivas NR, Hubbard JW, Quinn D, Midha KK. Enantioselective pharmacokinetics and pharmacodynamics of dl-threo-methylphenidate in children with attention deficit hyperactivity disorder. Clin Pharmacol Ther. 1992 Nov;52(5):561-8.
Effect of Racemate l-Methylphenidate did not affect locomotor activity in either lesioned rats or controls. d-Methylphenidate [ED(50)=1.66 mg/kg] was 3.3 times more potent than dl-methylphenidate [ED(50)=5.45 mg/kg] in reducing locomotor hyperactivity in lesioned rats • Davids E, Zhang K, Tarazi FI, Baldessarini RJStereoselective effects of methylphenidate on motor hyperactivity in juvenile rats induced by neonatal 6-hydroxydopamine lesioning. Psychopharmacology (Berl). 2002 Feb;160(1):92-8. Epub 2001 Dec 18.
Clinical Issues • Possible signal for skin sensitization with periods of use longer than the 6-week duration of the study. A skin exposure study of longer than 6-week duration would be helpful in investigating this potential signal. • Study showed sensitization occurred in 13-22%. Patients should not take MPH by any route again after sensitization.
Discussion Points • Total methylphenidate exposure will be greater for patch users; however this is almost completely due to the l-enantiomer. The long-term effects of this are unknown. • Short-term efficacy and safety were roughly comparable except for tics (MP 7%; C 1%); however, previous studies of larger patches with longer wear-times did not show an increase in tics over placebo (none reported- “twitching” 5% vs 0 placebo, but only 1/202 discontinuations). • The patch must be applied 2-hours before school and removed 9-hours after application. Use is more complicated; it may be removed prematurely or left on in error. • Is MP safe and effective when used as labeled? • Can MP be used as labeled in the population for which it is intended?