Download

1 / 44
500 likes | 1.16k Views
Correction of mid term assessement 4 sem. D Caroline Mohamed. Choose the single best answer. 26.About dental caries. Proximal surfaces Caries presents a broad area of origin and a conical, or pointed extension towards DEJ (inverted V shape).

E N D
Correction of mid term assessement 4 sem D Caroline Mohamed
Choose the single best answer 26.About dental caries. • Proximal surfaces Caries presents a broad area of origin and a conical, or pointed extension towards DEJ (inverted V shape). • Root-surface caries is more common in older patients it is U shaped in cross sections and it has a comparatively slow progression. • It is more difficult to arrest the progression of root caries than enamel caries because roots have a greater reuptake of fluoride than enamel. • Nursing bottle caries commonly occurs in the upper anterior teeth and rampant caries has the involvement of the mandibular teeth in the carious process. • All the answers are wrong • All the answers are right
Proximal surfaces Caries • The proximal surfaces are particularly susceptible to caries due to extra shelter provided to resident plaque owing to the proximal contact area immediately occlusal to plaque. • Lesion have a broad area of origin and a conical, or pointed extension towards DEJ. • V shape with apex directed towards DEJ. • After caries penetrate the DEJ softening of dentin spread rapidly and pulpally Dr.Caroline Mohamed
Characteristics of root caries: • Root caries lesions have less well-defined margins, tend to be U-shaped in cross sections, and progress more rapidly because of the lack of protection from and enamel covering. Dr.Caroline Mohamed
When the gingiva is healthy, root caries is unlikely to develop because the root surfaces are not as accessible to bacterial plaque. • The root surface is more vulnerable to the demineralization process than enamel because cementum begins to demineralize at 6.7 pH, which is higher than enamel's critical pH. • Regardless, it is easier to arrest the progression of root caries than enamel caries because roots have a greater reuptake of fluoride than enamel. Dr.Caroline Mohamed
Early childhood caries • Early childhood caries would include, two variants: Nursing caries and rampant caries. • The difference primarily exist in involvement of the teeth (mandibular incisors) in the carious process in rampant caries as opposed to nursing caries. Dr.Caroline Mohamed
27..About dental caries. • Radiotherapy is frequently associated with xerostomia due to decreased salivary secretion. • Pulp exposures and sensitive teeth are often observed in patients with acute caries. • The Chronic caries usually requires only prophylactic capping and protective bases. • Arrested caries involving dentin shows a marked brown pigmentation and induration of the lesion (the so called ‘eburnation of dentin’). • All the answers are wrong • All the answers are right Dr.Caroline Mohamed
Radiation caries • Radiotherapy is frequently associated with xerostomia due to decreased salivary secretion • This and other cause of decreased salivation may lead to a rampant form of caries, indicating the significance of saliva in preventing caries. Dr.Caroline Mohamed
Acute caries • Acute caries is a rapid process involving a large number of teeth. • These lesions are lighter colored than the other types, being light brown or grey, and their caseous consistency makes the excavation difficult. • Pulp exposures and sensitive teeth are often observed in patients with acute caries. • It has been suggested that saliva does not easily penetrate the small opening to the carious lesion, so there are little opportunity for buffering or neutralizaton Dr.Caroline Mohamed
Chronic caries • These lesions are usually oflong-standing involvement, affect a fewer number of teeth, and are smaller than acute caries. • Pain is not a common feature because of protection afforded to the pulp by secondary dentin • The decalcified dentin is dark brown and leathery. • Pulp prognosis is hopeful in that the deepest of lesions usually requires only prophylactic capping and protective bases. • The lesions range in depth and include those that have just penetrated the enamel. Dr.Caroline Mohamed
Arrested caries • Caries which becomes stationary or static and does not show any tendency for further progression • Both deciduous and permanent affected. • With the shift in the oral conditions, even advanced lesions may become arrested . • Arrested caries involving dentin shows a marked brown pigmentation and induration of the lesion (the so called ‘eburnation of dentin’). • Sclerosis of dentinal tubules and secondary dentin formation commonly occur. Dr.Caroline Mohamed
28. About caries risk . • Abdala is a 7 years old boy that leaves in AlMarge, a city with irregular levels of fluoride in the community water. He has 4 sisters and 2 brothers, his father is a truck driver and his mother is a housewife. He usually eats cakes and orange packaged juice at morning, traditional Libyan food at lunch and night and sometimes a chocolate between meals. He usually brushes his teeth at mornings.He is caries free. • We can infer by Abdala´s history that his risk for decay is low. • HIGH
b.Sumayais a 12 years old girl she leaves in Benghazi, a city where the levels of Fluoride in the water is irregular. She has 2 brothers and 1 sister, her mother is a teacher and her father is a police officer. She loves toffle chocolate sweets and regularly eats some between the meals. She is allergic to milk and milk derivate and suffers from Asthma. She brush her teeth twice a day. She presents oclusal pit and fissures caries on 26 and 36 and some cervical white spots on 34, 35, 44, 45. We can infer that Sumaya is on low risk of caries. High risk
MRS. Jumana, 56 years old, just had radiotherapy for treating a melanoma ( dermatological cancer) in her ear. She is caries free, rarely eats sweets and usually brushes her teeth twice a day. • We can infer by MrsJumanahistory that her risk for decay is high. • All the sentences are wrong. • All the sentences are right.
29. About periodontal disease • In phase IV, 7 to 11 days after initiation of plaque development, the diversity of the flora increases to comprise motile bacteria including spirochetes and vibrios as well as fusiforms and white blood cells appear. • The bacteria residing in the pocket and the host cells that defend it determine the clinical outcome. • In humans, when bacteria are allowed to accumulate in plaque on the tooth surfaces, enamel caries and gingivitis develop within 2 or 3 weeks. • The main sign of gingivitis is bleeding and periodontitis in the lost of periodontal insertion. • All the sentences are right • All the sentences are wrong
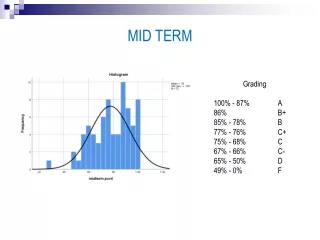
True and False questions: ( F )18. Dental caries has only one important causal factor that is the demineralization action of the acids produced by streptococosmutans. (F )19. When the pH at the surface of the tooth drops below 6.5, remineralization proceeds faster than demineralization (meaning that there is a net loss of mineral structure on the tooth's surface). This results in the ensuing decay. ( F )20. The white spot enamel lesion isn´t clinicaly visible but it is possible of remineralization. ( F )21.Adults continue to experience secondary dental caries, but they also experience a significant amount of primary caries around existing restorations. ( T )22.Xerostomia results in greater plaque accumulation and a reduced buffering capacity from the remaining saliva increasing the risk for dental caries and gingivitis. ( F ) 23. Among children, pit and fissure caries represent from 20 to 40% of all dental caries. ( T )24. Radiographs (bitewings) are needed for early discovery of proximal caries.
Host Educational level Socio-Economical Situation FLORA Fluoride in plaque Lactobacilli Oral Hygiene Streptococci Virulence factors Transmissibility HOST Age Fluoride Genetics Morphology Nutrition SUBSTRATE Carbohydrates Frequency of eating Oral clearance Physical nature of food Detergency of food SALIVA pH Flow rate Composition Buffering capacity Bicarbonate levels SALIVA Behavior Knowledge Dr.Caroline Mohamed
Tooth enamel dissolves at 5.5 ph D Caroline Mohamed
Tooth decay is caused by specific types of acid-producing bacteria that cause damage in the presence of fermentable carbohydrates such as sucrose, fructose, and glucose. • The mineral content of teeth is sensitive to increases in acidity from the production of lactic acid. Specifically, a tooth (which is primarily mineral in content) is in a constant state of back-and-forth demineralization and remineralization between the tooth and surrounding saliva. • When the pH at the surface of the tooth drops below 5.5, demineralization proceeds faster than remineralization (meaning that there is a net loss of mineral structure on the tooth's surface). This results in the ensuing decay. Dr.Caroline Mohamed
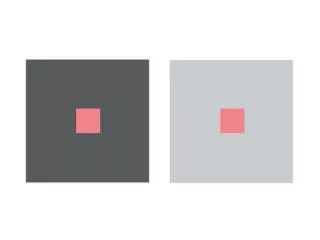
Incipient caries • The early caries lesion best seen on the smooth surfaces of the teeth, is visible as a ‘White Spot’ • Histologically, the lesion has an apparently intact surface layer overlying subsurface demineralization. • Significantly many such lesions can under go remineralization & thus the lesion is not an indication for restorative treatment • Remineralised with fluoride application • D/d: developmental defects of enamel Dr.Caroline Mohamed
Internal loss of minerals External (outer) surface White Spot Lesion: It is a subsurface lesion
Primary caries • A primary caries is one in which the lesion constitutes the initial attack on the tooth surface. • The designation of primary is based on the initial location of the lesion on the surface rather than the extent of damage. Dr.Caroline Mohamed
Secondary caries(Recurrent) • This type of caries is observed around the edges and under restorations. • The common locations of secondary caries are the rough or overhanging margin and fracture place in all locations of the mouth. • It may be result of poor adaptation of a restoration, which allows for a marginal leakage, or it may be due to inadequate extension of the restoration. • In addition caries may remain if there has not been complete excavation of the original lesion, which later may appear as a residual or recurrent caries. Dr.Caroline Mohamed
Radiation caries • Radiotherapy is frequently associated with xerostomia due to decreased salivary secretion • This and other cause of decreased salivation may lead to a rampant form of caries, indicating the significance of saliva in preventing caries. Dr.Caroline Mohamed
The occlusal surfaces of teeth represent 12.5% of all tooth surfaces but are the location of over 50% of all dental caries. Among children, pit and fissure caries represent from 80 to 90% of all dental caries. Pit and fissure caries can sometimes be difficult to detect. As the decay progresses, caries in enamel nearest the surface of the tooth spreads gradually deeper. Once the caries reaches the dentin at the dentino-enamel junction (DEJ), the decay quickly spreads laterally. Dr.Caroline Mohamed
Proximal caries are the most difficult type to detect. Frequently, this type of caries cannot be detected visually or manually with a dental explorer. • Proximal caries form cervically (toward the roots of a tooth) just under the contact between two teeth. As a result, radiographs (bitewings) are needed for early discovery of proximal caries. Dr.Caroline Mohamed
Q 4. Choose the right answer: • (paracetamol)(Substantivity );( );( tooth loss, tooth ache and pulpits) (ChlorhexidineDigluconate);( Fluoride sustained slow-releasing device • a)Paracetamol…is used to treat pain and to lower a high temperature but it does not help with inflammation. • d)Tooth loss, tooth ache and pulpits.. are some of the complications and sequelae of dental caries. • e) Substantivity…is defined as the ability of an agent to bind to tissue surfaces and be released over time, delivering an adequate dose of the active principle ingredient in the agent. • e)ChlorhexidineDigluconate……It´s more effective in preventing plaque accumulation on a clean tooth surface than in reducing preexisting plaque deposits.A disadvantage is brown staining of the teeth and the tongue after some weeks’ use particularly from mouthrinses. • f)Fluoride sustained slow-releasing device…is very helpful in reducing dental decay Dr.Caroline Mohamed
Q.7. Analyse these images and answer: • The MDF –T of this patient is …………..( Third molars not included)
Superior teeth D..2 M..2 F..5 Decayed Restored Restored Restored Decayed Restored Restored Missed Missed
Inferior teeth D..0 M..2 F..4 Missed Missed Filled Filled Filled Filled
The gingival index of this patient is……Moderate 2
Gingival Index: GI 0 1 2 3
c) The calculus index of this patient is …4/ Heavy
Sign the worse score Sign the worse score Sign the worse score Choose the worse score