Download
1 / 101
1.05k likes | 1.19k Views
Presented by Dr. Fadel Naim, this resource covers the evaluation of neurovascular function post-fracture, mechanisms of musculoskeletal injury, and classification of fractures. Explore the impact on bone and soft tissues, assessment guidelines, and importance of diagnosing open fractures promptly. ###

E N D
General Principles of Fracture Care Presented By: FadelNaim M.D. Orthopedic Surgeon Faculty of Medicine IUG
Fracture • The problem is not the damage to the bone • The problem is the damage the bone does to the surrounding soft tissues. • Evaluate Neurovascular Function Distally
Fracture • A disruption in the integrity of a living bone involving injury to: • Bone • Bone marrow • Periosteum • Adjacent soft tissues
Mechanisms of Musculoskeletal Injury • Direct force • Indirect force • Twisting (rotational) force
Direct trauma: • Consists of direct force applied to the bone • Tapping fractures (eg, bumper injury) • Penetrating fractures (eg, gunshot wound) • Crush fractures
Indirect trauma • Involves forces acting at a distance from the fracture site • Tension (traction) • Compressive forces • Rotational forces
Indirect Trauma Rotation Tension Compression Combination Angulation
ClassificationofFractures • Evidence based medicine • Communication • Treatment plan (personality of the fracture...)
Fracture Discription • Anatomical location - ? joint • Direct / indirect • Fracture configuration • Simple or comminuted • Open or closed • Pathological • Stress fracture • Greenstick fracture
The Rule of A's Radiographs should be described as follows: • Anatomy (eg, proximal tibia) • Articular (eg, extra-articular) • Alignment (eg, first plane) • Angulation (eg, second plane) • Apex (eg, apex pointing medially) • Apposition (eg, 75% or 0%)
Anatomical and Clinical Discreption Epiphysis Physis • Which bone? • Thirds (long bones) • Proximal, middle, distal third • Anatomic orientation • E.g. proximal, distal, medial, lateral, anterior, posterior • Anatomic landmarks • E.g. head, neck, body / shaft, base, condyle • Segment (long bones) • Epiphysis, physis, metaphysis, diaphysis Metaphysis Diaphysis (Shaft) Articular Surface
Anatomical and Clinical Discreption Articular Extension / Involvement • Intra-articular fractures • “Involves the articular surface” • Dislocation • Loss of joint surface / articular congruity • Fracture-dislocation
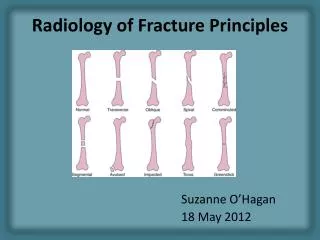
Comminution / Pattern • Transverse (Simple) • Oblique (Simple) • Spiral (Simple) • Linear / longitudinal • Segmental • Comminuted • Compression / impacted • “Buckle / Torus” • Distraction / avulsion
Displacement, Angulation, Rotation • Displacement • Extent to which Fx fragments are not axially aligned • Fragments shifted in various directions relative to each other • describe displacement of distal fragment relative to proximal Oblique tibial shaft Fx b/w distal & middle thirds; laterally displaced
Displacement, Angulation, Rotation • Angulation • Extent to which Fx fragments are not anatomically aligned • In a angular fashion • describe angulation as the direction the apex is pointing relative to anatomical long axis of the bone (e.g. apex medial, apex valgus) R Tibial shaft Fx b/w prox & middle thirds, angulated apex lateral (apex varus)
Displacement, Angulation, Rotation Angulation Valgus Apex medial Parallel No angulation Varus Apex lateral
Displacement, Angulation, Rotation • Rotation • Extent to which Fx fragments are rotated relative to each other • Convention: • describe which direction the distal fragment is rotated relative to the proximal portion of the bone
Displacement, Angulation, Rotation Rotation • PA view of rotated hip Fx • Greater trochanter perpendicular to film • Normal PA view of hip • Greater trochanter in profile
Displacement, Angulation, Rotation Shortening • Has the fracture caused shortening of the bone involved? • To what extent has shortening occurred?
Intrinsic Bone Quality Normal • Osteopenia • Decr’d density
Intrinsic Bone Quality • Osteopetrosis • Incr’d density Normal
Intrinsic Bone Quality Normal • Osteopoikilosis • Focal areas of incr’d density
Soft tissue involvement • Is the fracture open or closed? • Is associated neurological and or vascular injury present? • Is there muscle damage or compartment syndrome evident?
Open fracture implies communication between external environment and the fracture. • A soft tissue injury complicated by a broken bone.
Components of open fracture • Fracture • Soft-tissue damage • Neurovascular compromise • Contamination • Extent of each component must be assessed individually in order to achieve a comprehensive understanding of the injury, upon which the treatment plan can be based.
Gustilo and Anderson Classification • Model is tibia, however applied to all types of open fractures • Emphasis on wound size • Crush injury assoc with small wounds • Sharp injury assoc with large wounds • Better to emphasize • Degree of soft tissue injury • Degree of contamination
Why use this classification? • Grades of soft tissue injury correlates with infection and fracture healing
Nocosomial infection?!!!! Cover the wounds quickly • Only 8% of infections were caused by the same organism initially isolated in the perioperative cultures • 92% of open fracture infections were caused by bacteria acquired while the patient was in the hospital
Gustilo Classification of Open Fracture • Type I: • Wound is shorter than 1 cm. • It is clean and generally is caused by a fracture fragment piercing the skin (ie, inside-out injury). • This is a low-energy injury.
Gustilo Classification of Open Fracture • Type II: • The wound is longer than 1 cm. • It is not contaminated and without major soft tissue damage or defect. • This is also a low-energy injury.
Gustilo Classification of Open Fracture • Type III: • Wound longer than 1 cm, with significant soft tissue disruption • High-energy trauma resulting in a severely unstable fracture with varying degrees of fragmentation • IIIa: • Sufficient soft tissue to cover the bone without the need for local or distant flap coverage
Gustilo Classification of Open Fracture • Type III: • IIIb: • Extensive soft tissue disruption • Local or distant flap coverage is necessary to cover the bone • The wound may be contaminated, and serial irrigation and debridement procedures are necessary to ensure a clean surgical wound
Gustilo Classification of Open Fracture • Type III: • IIIc: • Any open fracture associated with an arterial injury, which requires repair is considered type IIIC • Involvement of vascular surgeons is generally required
Gustilo Classification of Open Fracture • Type I: • Wound is shorter than 1 cm. • It is clean and generally is caused by a fracture fragment piercing the skin (ie, inside-out injury). • This is a low-energy injury. • Type II: • The wound is longer than 1 cm. • It is not contaminated and without major soft tissue damage or defect. • This is also a low-energy injury. • Type III: • Wound longer than 1 cm, with significant soft tissue disruption • High-energy trauma resulting in a severely unstable fracture with varying degrees of fragmentation • IIIa: • Sufficient soft tissue to cover the bone without the need for local or distant flap coverage • IIIb: • Extensive soft tissue disruption • Local or distant flap coverage is necessary to cover the bone • The wound may be contaminated, and serial irrigation and debridement procedures are necessary to ensure a clean surgical wound • IIIc: • Any open fracture associated with an arterial injury, which requires repair is considered type IIIC • Involvement of vascular surgeons is generally required
I IIIA II IIIB IIIC
Clinical Manifestations of fracture • Edema • Pain and Tenderness • Muscle spasm • Deformity • Ecchymosis • Loss of Function • Crepitation
The six “P”s of musculoskeletal assessment • Pain • on palpation • on movement • constant • Pallor - pale skin or poor cap refill • Paresthesia - “pins and needles” sensation • Pulses - diminished or absent • Paralysis • Pressure
Pre-reading Musculoskeletal Radiographs • 1: Name, date, old films for comparison • 2: What type of view(s) • 3: Identify bone(s) & joint(s) demonstrated • 4: Skeletal maturity (physes: growth plates) • 5: Soft tissue swelling • 6: Bones & joints (fractures & dislocations)
Reading X-rays • Say what it is- • what anatomic structure are you looking at • how many different views are there • Regional Location- • Diaphysis (rule of 1/3) • Metaphysis • Epiphysis including intra and extra-articular • Direction of the fracture line- Transverse, Oblique, Spiral
Reading X-rays • Condition of the bone- • comminution (3 or more parts) • Segmental (middle fragment) • Butterfly segment • Incomplete • Avulsion • Stress • impacted • Deformity • Displacemtent (distal with respect to proximal) • angulation (varus, valgus) • Rotation • shortening (in cm’s) • distraction
Diagnosis of FractureX-RayThe Rule of 2s • Two views: • Anteroposterior (AP) and lateral views of the injured limb (2 views 90° orthogonal to each other) • Two joints: • The joint above and the joint below the injury • Two limbs: • Radiographs of both the injured and noninjured limbs especially in children with epiphyseal-plate injuries • Two times: • 1 prereduction image and 1 postreduction or postfixation image
CT Scanning Not indicated for routine evaluation of common fractures • Preoperative planning for complicated fractures • Provide information about the architecture of fracture lines especially about intra-articular fractures • Evaluate severely fragmented fractures and those involving the epiphyseal segment • Is indicated in assessing the spinal column for injury
Fracture Healing • Primary healing • Non displaced fractures, fractures with compressive fixation across the fracture site • Osteoblasts traverse the fracture site and lay down lamellar bone without forming immature bone when there is direct contact between cortical bone ends
Fracture Healing • Secondary healing • No compression across fracture site, motion can occur • Fracture callus forms to stop motion, stage of consolidation and remodeling