
BURNS
E N D
Presentation Transcript
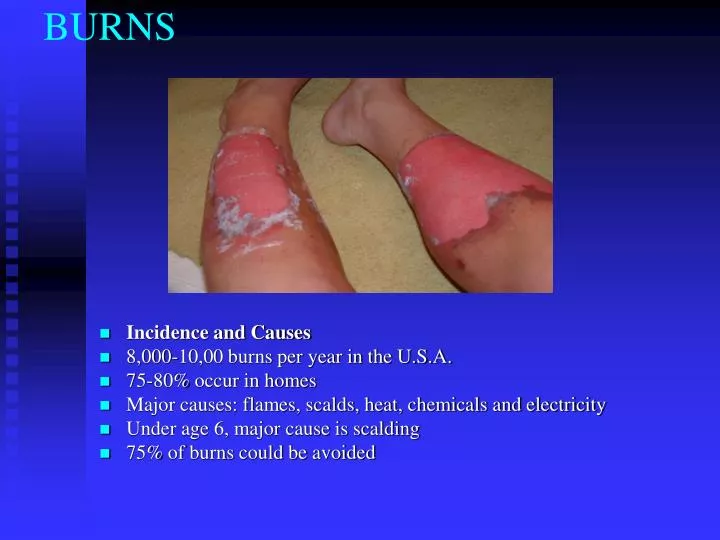
BURNS • Incidence and Causes • 8,000-10,00 burns per year in the U.S.A. • 75-80% occur in homes • Major causes: flames, scalds, heat, chemicals and electricity • Under age 6, major cause is scalding • 75% of burns could be avoided
Emergent Care • Burning process stopped with removal of clothing, jewellery and covering affected area with cool water • Increase blood volume with IV inserted in intact skin area • Urinary catheter to monitor fluid output, indicates dehydration • Intubation to secure an airway • Vitals; BP, HR, BPM, Temp • Determining extent of damage; Rule of Nines or Lund -Browder
Body surface affected (BSA) • The Rule of Nines • Entire head = 9% • Each arm = 9% (18%) • Chest = 9% • Abdomen = 9% • Upper back = 9% • Lower back = 9% • Front of each leg = 9% (18%) • Back of each leg = 9% (18%) • Groin = 1% • Total 100% • This along with the cause of the burn helps determine the severity of the burn
Lund-Browder • Accurate assessment of TBSA
Complications of Major Burns • Pulmonary injury; Stridor (whistling) with breathing • Hypovolaemia; loss of plasma and decreased BP • Hypothermia; with skin gone there is no thermoregulation • Cardiac Arrhythmia; irregular heart beat. • Kidney Failure • Death
When burns are critical • Any burn greater than 25% BSA • Full or deep-partial-thickness burns greater than 10% BSA • Burns complicated by a respiratory or airway injury • Most burns involving the face, hands, feet or genitals • Burns complicated by a fracture or major soft-tissue injury • Electrical or deep-chemical burns • Burns occurring in patients with serious pre-existing medical conditions
Classification of Burns • First degree or superficial burns involve only the epidermis; • burned area is red; no blisters. • Second degree or partial thickness burns involve all of epidermis & varying depths of the dermis. • Appearance -blisters, pink, moist, Extremely painful. • Third degree or full thickness burns involve epidermis & entire dermis, possible deeper tissue such as muscle and bone. • Appearance- white and dry. May be free of pain. Requires skin grafting.
Burn types • Thermal - most common (Other than sunburn) • direct flame, scalds and direct contact. • Chemical - contact strong acids or alkalis. • burning process continues as long as the chemical, or agent, is on the body. • need to know the specific chemical because the treatment must be specific • Electrical - type I, II and III. • Type I - contact burn - most common - true electricity injury. burn is most severe at the entry and exit points. • Type II - flash burn - victim becomes part of an electrical arc. • Type III - flame burn- electricity ignites the victim's clothing. • Sunburn. Radiation burns are by far the most common burns because of being exposed to an enormous nuclear reactor, the sun. • sunburns are almost always superficial. • Don't underestimate the potential severity of sunburn. Using the Rule of Nines, it is not uncommon for sunburn to reach the critical stage (burns greater than 25 percent BSA), • Some patients require skin grafting after prolonged sun exposure.
Burn treatment • 1.stop the burning • 2. evaluate the injury • 3. relieve pain • 4. prevent shock • 5. infection. • Even though the fire is out, the burning can continue. • Remove all burned clothing • flush the skin with cool water. • Flushing is crucial to a chemical burn, particularly alkalis which must be flushed for 1 to 2 hours • Burned skin loses heat more rapidly than intact skin and cool water can cause hypothermia if a large BSA has been burned. • Pay particular attention to the airway. An airway problem may not be immediately apparent. • If the patient has airway involvement or any respiratory difficulty, advanced rapid treatment is required. • Superficial burns are easily managed with cool compresses and acetaminophen for the pain. • An extensive superficial burn will demand a slightly stronger analgesic and should be accompanied by an increase in fluid intake by the patient. • basic systemic pain control along with fluid intake is the best approach. • treatment of partial-thickness burns follows the same approach of cooling the area and covering the burn with a sterile dressing. • Do not break the blisters; they are actually the best burn dressing available. If the blisters rupture later, apply Silvadene as an antibiotic ointment and cover with dry, sterile dressing. • Fluid loss can be an early complication and is most common with partial-thickness and deeper burns. • Depending on the extent of BSA involved, a fluid loss can rapidly lead to shock. • If the BSA is greater than 15 percent, fluid replacement is required. This is best managed with I-V fluids




















