Download
1 / 48
510 likes | 1.2k Views
Nutrition and Bowel Elimination. Lee Resurreccion Unit 9, Part 1. Assessment of Digestive and Gastrointestinal Function: Chapter 34. Lee Resurreccion Unit 9, Part 1. Organs of the Digestive System. Components to the GI System. Mouth Pharynx Esophagus Stomach Small intestine

E N D
Nutrition and Bowel Elimination Lee Resurreccion Unit 9, Part 1
Assessment of Digestive and Gastrointestinal Function:Chapter 34 Lee Resurreccion Unit 9, Part 1
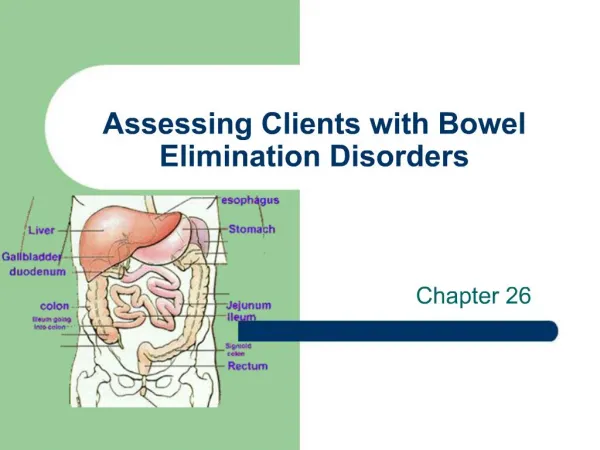
Components to the GI System • Mouth • Pharynx • Esophagus • Stomach • Small intestine • Large intestine • Liver- associated organ • Biliary Tract- associated organ • Pancreas-associated organ
Primary Functions of the G.I. Tract • Ingestion • Mouth, pharynx, esophagus • Digestion • Mouth, stomach, small intestine • Absorption • Small intestine • Elimination • Large intestine
Major Enzymes and Secretions • Mouth: saliva, salivary amylase • Stomach: hydrochloric acid, pepsin, intrinsic factor • Small intestine: amylase, lipase, trypsin, bile • See Table 34-1
G.I. Tract Innervation • Innervated by autonomic nervous system • Sympathetic (inhibitory) • Parasympathetic (excitory) • Intrinsic nervous system (gut brain) • Coordinates motility and secretion • Receives 25-30% cardiac output
Mouth, Pharynx, Esophagus, Stomach • Mouth • Mechanical and chemical functions • Pharynx • Secretes mucus • Esophagus • Muscular, peristaltic contractions • Stomach • Mechanical and chemical functions
Small Intestine • Composed of the duodenum, jejunum and ileum • Fingerlike projections called villi • Goblet cells that secrete mucus • Epithelial cells that produce digestive enzymes • Fats to glycerol and fatty acids • Proteins to amino acids • Carbohydrates to monosaccharides • Additional secretions from pancreas and liver (later slides)
Large Intestine • Four components • Cecum and appendix • Colon • Rectum • Anus
Large Intestine (Continued) • Contains microorganisms • Functions: • Absorption of water and electrolytes • Formation feces • Reservoir for fecal mass until defecation
The Liver • Largest internal organ • Four major functions • Metabolic-carbs, fat, protein, and metabolism of certain drugs • Bile synthesis • Storage-glucose in the form of glycogen, vitamins, minerals and amino acids • Phagocyte system • Functional units - lobules
Biliary Tract • Bile drains to gallbladder via right/left hepatic ducts • Gallbladder: • Concentrates and stores bile • Releases bile into the cystic duct to the common bile duct into the duodenum at the ampulla of Vater
The Pancreas • Exocrine cells secrete pancreatic enzymes • Endocrine function • Beta cells
Assessment: History • Include all information related to GI function • Abdominal pain, dyspepsia, gas, nausea and vomiting, constipation, diarrhea, fecal continence, change in bowel patterns, characteristics of stool, jaundice, history of GI surgery or problems, appetite and eating patterns, teeth, and nutritional assessment, including weight patterns • Psychosocial, spiritual, and cultural factors • Assess knowledge; need for patient education
Subjective Data PMH Meds Surgeries Health Practices Maintenance Elimination Sleep Exercise Objective Data Inspection Auscultation Must do prior to palpation! Percussion Palpation Assessment of the GI System
Diagnostic Tests • Stool specimens • Breath tests • Abdominal ultrasound • Imaging studies: CT, PET, MRI • Upper GI tract study • Lower GI tract study • GI motility studies • Endoscopic procedures • Other
Disorders of the Esophagus • Dysphagia • Achalasia • Diffuse spasm • Hiatal hernia • Perforation • Foreign bodies • Chemical burns • GERD (gastroesophageal reflux disease) • Esophageal cancer
Upper GI Complications • GERD • Hiatal hernia • CA
Gastroesophageal Reflux Disease(GERD) Causes: • Impaired motility of the esophagus • Delayed gastric emptying • Defective defenses of the esophagus • Dysfunction of the lower esophageal sphincter (LES)
GERD (continued)Signs/Symptoms • Heartburn (pyrosis) • Regurgitation • Sore throat • Bloating • Dyspnea/wheezing or coughing
GERDComplications • Esophagitis resulting in stricture formation • Dysphagia • Barrett’s esophagus • Potential pulmonary complications
GERD (continued)Signs/Symptoms • Heartburn (pyrosis) • Regurgitation • Sore throat • Bloating • Dyspnea/wheezing or coughing
GERD Non-Surgical Therapy • Lifestyle modifications • Smoking cessation • PO intake and timing of intake • Medications: • Antacids • Antisecretory • H2 antagonists (discussed later) • Proton pump inhibitors (discussed later)
GERD Surgical Therapy • Objective: to restore gastroesophageal integrity • Last resort • Laproscopically performed • LES is reinforced by wrapping stomach tissue around esophagus
Hiatal Hernia Pathophysiology • Structural changes • Weakening muscles of diaphragm • Increased intraabdominal pressure • Obesity/pregnancy/ascites/tumors/physical exertion • Age • Poor nutrition • Prolonged illness (confined to bed)
HiatalHernia Signs/Symptoms • Similar to GERD • Mimics gallbladder disease, peptic ulcer and angina • Some patients experience no symptoms. • Symptoms precipitated by large meals, alcohol and smoking • Bending over may cause severe burning pain, relieved by sitting or standing • Nocturnal attacks are common
Hiatal HerniaComplications • Hemorrhage from erosion • Stenosis • Ulcerations of herniated portion of stomach • Strangulation of the hernia • Regurgitation with tracheal aspiration • Severe chronic esophagitis following reflux problem (GERD)
Hiatal HerniaNon-Surgical Therapy • Antacids • Antisecretory agents • Elimination of constricting garments • Avoidance of lifting and straining • Elimination of alcohol and smoking • Elevation of the head of bed
Hiatal HerniaSurgical Therapy • Primarily laproscopically performed • Goals • Decrease the hernia • Increase LES pressure • Prevent movement of the gastroesophageal junction • Similar to GERD surgical procedures • Last resort
Nursing ManagementGERD/Hiatal Hernia • Assessments • Interventions • Diet • HOB elevated • Weight reduction (if appropriate) • Emotional support • Meds
Cancer of the Stomach • No single causative agent has been identified • Diets containing smoked, highly salted, or spiced foods may have a carcinogenic effect. • Possible genetic etiology • Blood group “A” has a greater incidence than general population • Non-specific mucosal injury, resulting in chronic gastritis. Proliferation of H. pylori and metabolic changes induces transition from dysplasia to carcinoma
Anemia caused due to chronic blood loss or pernicious anemia Pale Weak Complains of fatigue Pain and discomfort sometimes identical to those of peptic ulcer disease Alleviated by belching and by use of antacids, antisecretory agents and diet modification Indigestion, epigastric fullness, early satiety, weight loss, dysphagia and constipation Gastric CASigns/Symptoms
Gastric CA Therapy • Surgery • Subtotal gastrectomy • Total gastrectomy with esophagojejunostomy ( see diagram) • Adjuvant therapy • Radiation therapy • Chemotherapy • Combination radiation and chemotherapy
An incision is made in the skin over the pyloric region of the stomach.
Gastric CA (continued)Dumping Syndrome • Direct result of removal of large portion of the stomach and pyloric sphincter • Usually occurs 15-30 mins after meal and last ~1 hour • Pt c/o urge to defecate, weakness, sweating, palpitations and dizziness
Nursing ManagementGastric CA • Assessments • Interventions • Pre and postop procedures • Emotional support • Teaching • Minimizing dumping syndrome • Postprandial hypoglycemia • Postop teaching (incision, pain, diet, activity)