Download
1 / 102
1.02k likes | 1.29k Views
Resurgence of diphtheria in East Java where do we are ?. Ismoedijanto Balai besar Laboratorium kesehatan Surabaya, 09 10 2012. Propinsi versus kabupaten /kota …………………….kecuali yang melakukan ORI…. . KKK (kemana kemkes kita)…........ Hehehe….. Mohon maaf lahir batin.

E N D
Resurgence of diphtheria in East Java where do we are ? Ismoedijanto BalaibesarLaboratoriumkesehatan Surabaya, 09 10 2012
Propinsi versus kabupaten /kota…………………….kecuali yang melakukan ORI…. KKK (kemana kemkes kita)…........ Hehehe….. Mohon maaf lahir batin
some view of a clinician • Difterisebagaipenyakitmenular (Clinical site) • Gambaranklinik, komplikasidanpengobatan • Difteri as one of VPD (vaccine preventable disease) • Mencegahkesakitan, kematiandankomplikasi • Imunisasiimunogendifteri • difteri serve as one of the indices • Indikator health services • Indikatorimunization services
Report and presentation on East Java diphtheria • Presentasi KLB difteri Bangkalan th 2005 di ACPID (Asian Congress of Pediatric Infectious Disease) ke 3, Cebu Philipina • Diramalkan menjadi klb pada PIT IDAI th 2007, Yogyakarta • Pertemuan imunisasi, SO Jawa Timur 2007 • Pertemuan SO ttg PD3I, Makassar 2008 mengingatkan difteri • Laporan KLB diferi Jawa Timur di KONIKA /ACPID 4, 2008, di Surabaya • Meeting TAGI 2008,2009, ( rekomendasi Td ) , Satgas Imunisasi IDAI 2009, 2010 , pertemuan Kemkes selama th 2009, 2010 , (tidak ada tahun 2011), bandung , denpasar , jakarta , bogor. Belum menjadi masalah, kedua terbanyak di dunia • Pertemuan SO Batam october 2011, Bandung 2011
WHO ELIMINATION GOAL FOR DIPHTHERIA “The target for European member states was the elimination of indigenous diphtheria by the year 2000. This meant the absence of indigenous cases caused by toxigenic Corynebacterium diphtheriae strains.” Ten years past the elimination target date and the elimination goal has not been met. Indigenous transmission continues: Latvia, Ukraine, Lithuania, Russian Federation and other NIS countries. Sporadic cases: EU member states. Cases and large epidemics are still occurring in other parts of the world, South East Asia (Indonesia, India), Africa, Eastern Mediterranean, South America. EPIDEMIC DIPHTHERIA IS STILL WITH US
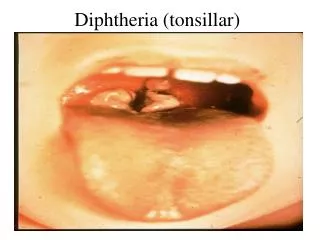
Clinical picture of diphtheria Gejala, tatacara diagnosis, komplikasi
Gambaran klinik Diphtheria • Masa Inkubasi 2-5 days (range, 1-10 days) • Tanda utama • Ada pseudomembran • Menghasilkan toksin • site of infection • Anterior nasal • Tonsillar and pharyngeal • Laryngeal • Cutaneous • Ocular • Genital
MANIFESTASI KLINIK • Variasi gejala: tanpa gejala hipertoksik & fatal • Faktor-faktor: • primer: imunitas, virulensi • toksinogenesitas., lokasi anatomis • lain-lain: umur, peny sistemik penyerta, kepadatan hunian, peny pada nasofaring • Masa tunas: 2-6 hari • tanda klinik : • Demam <38,50 C , tidak tinggi • nyeri telan • Membaik dalam 5 hari
Other complications • Palatum molle paralisis • Paralisis saraf kranial: diplopia, strabismus • Paralisis saraf perifer: tangan, kaki • Acute kidney injury • Endocarditis • Arthritis • osteomyleitis
Medical management (1) • Umum: • istirahat mutlak ±2 minggu, • cairan/ diit adekuat, • jaga nafas tetap bebas, lakukan trakheostomi bila: gelisah, iritabel & gangguan pernafasan progresif • komplikasi • Lakukan sonda nasogastrik bila ada paralisis palatum molle • Tatalaksana miokarditis • Tatalaksana AKI • Tatalaksana paralisis
Medical management (2) • Khusus: • karena toksin menyebabkan kerusakan sel, perlu segera diberikan antitoksin/antibodi, karena penderita tidak mempunyai antibodi • -antitoksin; serum anti difteri (ADS) segera secara intramuskuler (kadar maksimal tercapai setelah 4 hari) atau intravena diencerkan dalam 200 ml garam faali dan diberikan selama 4 jam, sediakan adrenalin 1:1000 dalam semprit, kortikosteroid; didahului tes kulit/tes konjungtiva • Dosis ADS: 20.000 – 120.000 KI : • 20.000 ringan difteri nasal dan permukaan • 60.000 sedang : beslag sedang • 100.000-120.000 berat: beslag luas, bullneck,toksik
Dosage of anti-toxin Details in HPA Immunoglobulin handbook available at: http://www.hpa.org.uk/infections/topics_az/immunoglobulin/pdfs/diphtheria.pdf
-antimikrobial: untuk menghentikan produksi toksin • Procain penic 50.000 – 100.000 KI/Kg/hari atau eritomisin 50 mg/Kg/hari selama 10 hari • -kortikosteroid: kontroversi • -pengobatan penyulit: • terutama ditujukan menjaga hemodinamika tetap baik • mengatasi gangguan fungsi pompa jantung • NGT pada paralisis palatum mole • Mengatasi gangguan fungsi ginjal • Pengobatan paralisis perifer
Diagnosis and outbreak • Hanya 40% penderitadengankultur pos ok: • Mendapatantibiotika • Salahcarapengambilanmisditengahbeslag • Salah media pertumbuhan • Salahtatacarakirim • Adanyakuman lain • Adanyakasusygterlambat, sudahdengankomplikasi (miokarditis), beslagsdhhilang • Culture proven dantoxigenicity test • PCR dengan swab • Makin langkanya expertise • Overdiagnosiskasusterutamakasusdewasa
Source of reports TAHUN 2010 - 2011 DPS DPS PKM PKM RS RS 2010 2011
TREND BULANAN KASUS DIPHTERI DI JATIM 2008 – 2011 ( 20 SEPT 2011 ) PascaIdulfitri
DISTRIBUSI KLB DIPHTERI DI JATIM TH 2000–2011 665 Jml Mati Tahun
SEBARAN DIPHTERI DI JATIM s/d 9 November 2012 20/1 7 27 28/1 3 17/1 6 7/1 65/1 21 22 5 89/11 4 7 3 117/7 4 5 8 26 18/1 10 12 23/1 19/1 2 31 8 17 1 14 12 50/2 17 6 7 5 16/1 N : 31 N = 31 Jmlkasus = 762 Jml mati = 29 Jmlkab/ko = 38 (16 Mei ) WIL SUB PIN 2012
SEBARAN “ C difteriae – Toxigenic “ PADA KLB DIPHTERI DI JATIM s/d 14 Juni 2012 Mapping Area C. diphtheria Patogenic & Toxigenic in East Java 2011 -2012 M+B M+I M+G M M M+B M M M M M M M+B M M M+B M+B M M+B M M • C difteri var. • Mitis (M) • Gravis (G) • Intermedius (I) • Belfanti (B) Data & Informasi BBLKSUB 2012
KASUS DIPHTERI DAN IMUNISASI DPT3 – DT-SD DI JAWA TIMUR s/d Jan 2010 DT-SD DPT3 KASUS DIPHTERI bwk keren
Case definition • Clinical case: • Sore throat • Pseudomembrane • Kulit/conjunctiva/mukosalainnya • Probable: • Clinical case • Contact or linked to confirmed case • Confirm case: • Probable/clinical • Pos culture and toxigenic
case definitions /clinical criteria WHO • respiratory • and • pseudomembrane • EU • respiratory • nasal • cutaneous • other sites
Peran lab untuk kasus KLB WHO • Isolation of C diphtheriae • or • 4-fold rise in antibody titre • EU • Isolation of toxin producing C.diphtheriae or C.ulcerans
arti non-toxigenic C.diphtheriae • Severe infections with non-toxigenic C.diphtheriae have been documented • Namun , isolates sering didapat pula dari px le pharyngitis, sometimes with other organisms • No need for clearance swabs or contact tracing • Menjadi toxigenic bila terinfeksi bacteriophage dg gene tox pos
Enhanced surveillance of laboratory confirmed toxigenic corynebacterium infections
SEBARAN “ C difteriae – Toxigenic “ PADA KLB DIPHTERI DI JATIM s/d 14 Juni 2012 Mapping Area C. diphtheria Patogenic & Toxigenic in East Java 2011 -2012 M+B M+I M+G M M M+B M M M M M M M+B M M M+B M+B M M+B M M • C difteri var. • Mitis (M) • Gravis (G) • Intermedius (I) • Belfanti (B) Data & Informasi BBLKSUB 2012
POSITIV RATE SPESIMEN DIFTERI HASIL PEMERIKSAAN LAB. DI JATIM TAHUN 2011 POSITIV RATE (%)
Performance of Diphtheria Laboratory By Outbreak Specimens 2005-2011 Positiv rate (%)
Epidemiological managementto stop transmision dan immunization
Tatalaksana epidemiologik • Isolasi ketat / barrier nursing: difteri sangat menular • Tatalaksana kontak untuk mencegah penyebaran: • Dewasa: identifikasi sebagai sumber penularan dan obati bilamana kultur pos • anak/saudara: • Amati bila dalam masa inkubasi : penderita baru • Tanpa gejala, imunisasi lengkap: booster • Tanpa gejala, imunisasi tak lengkap/tak imunisasi: imunisasi dasar dan booster • Kultur pos: obati • Erytromisin etilsuksinat untuk menekan circulating C diphtheria • Imunisasi penderita setelah sembuh .
Epidemiology of diphtheria: Prevaccine era • highly endemic childhood disease in temperate climates • most acquired immunity by 15yrs, few adult cases • approx. 85% developed immunity from mild or asymptomatic infection, only 15% typical clinical diphtheria • gradual decline in deaths • was still one of leading causes of childhood death until widespread vaccination implemented
Screening kekebalan dan Tata Laksana Tes Shick pos berarti anak rentan, negatif anak kebal
mengapa ada yang tidak kebal • Sebelum vaccine era transmisikumansangatkuat, sehinggadapatmenimbulkankekebalanalamiah • Transmisiberkurangakibat • Perbaikansanitasidanlingkunganhidup • kekebalanmanusiaakibat vaccine • Kegagalanimunisasi • Tidakimunisasi • Gagalimunisasi • Cakupankurangtinggi • Cakupan SIA (supplementary Immunization Activity) harustinggi ok • Spill over IgGdi tonsil • Membuatkasusmenurun
Prevention and control of diphtheria • Routine vaccination • Surveillance • Case management • Management of close contacts • Outbreak management • Social interventions
Diphtheria cases*, deaths, and vaccine coverage England and Wales: 1914 to 2005 Immunisation *notifications up to 1985, laboratory confirmed cases 1986 to 2005
Apa yang perlu dilakukan Ja Tim • Menekan kematian kasus (short term) • Deteksi dini dan rujukan • Manajemen kasus • Menekan transmisi & kasus baru (short term) • PE • ORI di daerah kasus • Mencegah KLB (long term) • Meningkatkan cakupan • Meratakan cakupan, meniadakan kantong