Download
1 / 55
910 likes | 2.97k Views
PT 142: Assessment in Physical Therapy Introduction to Musculoskeletal/ Orthopedic Assessment. Aila Nica J. Bandong, PTRP Instructor Department of Physical Therapy Clinical Supervisor CTS-Pediatric Section UP-College of Allied Medical Professions. Learning Objectives.

E N D
PT 142: Assessment in Physical TherapyIntroduction to Musculoskeletal/Orthopedic Assessment Aila Nica J. Bandong, PTRP Instructor Department of Physical Therapy Clinical Supervisor CTS-Pediatric Section UP-College of Allied Medical Professions
Learning Objectives At the end of the lecture, the student should be able to: • Determine the principles and concepts of a musculoskeletal assessment • Identify cues and information that needs to be obtained in a subjective musculoskeletal assessment • Formulate hypothesis of the problems assessed and determine examination procedures that may confirm or refute a hypothesis
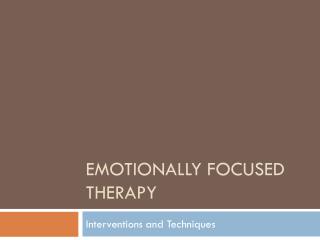
Model of Orthopedic Dysfunction Systemic Disease Emotional Tension Body System Lesion Stimulus Infection Physical Trauma Internal Tissue Response Immediate Tissue Insufficiency
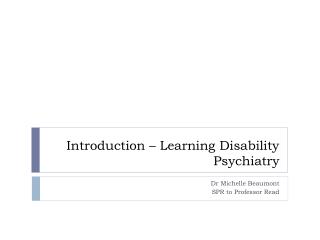
Altered Mechanical Properties of Tissues and Structure Internal Tissue Response Immediate tissue insufficiency Pain Inflammation Vasodilation Altered Internal Tissue Stress Swelling Contractile Noncontractile Tissue Irritation Internal tissue Ischemia Functional Soft Tissue Contracture
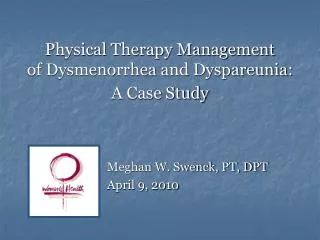
Altered Mechanical Properties of Tissues and Structure Swelling Immobilization Altered Internal Tissue Stress Non-Contractile Tissue Contractile Tissues Fibrous Reaction Soft tissue Contracture Intrinsic Tissue Insufficiency Altered Myotendon Unit Composition and Dynamic Function Articular Structures Acquired Tissue Insufficiency Altered alignment of joint Altered Arthrokinematics Altered Osteokinematics
Why perform a comprehensive examination? • Establish a sound therapeutic relationship with the patient • Make a clinical diagnosis • Identify the goals or outcome of physical therapy management • Establish a set of baseline data and measurement procedures that can be used to judge treatment outcomes • Establish the presence of any contraindications or precautions to treatment • Identify the most appropriate intervention strategy to achieve goals • Decide upon the dose of the appropriate strategies or treatments that will be effective in achieving goals
Components of a Comprehensive Musculoskeletal/Orthopedic Assessment
Demographic Data • Name • Age • Occupation – identify work requirements • Repetitive movements • Position of limb at work • Recreational pursuits/ sports • Activities of daily living • Gender • Marital status • Address • Nationality • Handedness
Date admitted ( for in-patients ) Admitting unit ( for in-patients ) Attending physician Date evaluated Date of initial evaluation Working diagnosis Demographic Data
Subjective Assessment • Area and type of symptoms • Current history/ mechanism of injury • 24-hour pain behavior • Aggravating and alleviating factors • Past history of the condition (if any) • Past medical history • Family medical history • Personal/Social history • Ancillary procedures • Medications • Chief complaint • Previous treatment and effect (if any)
AREA AND TYPE OF SYMPTOMS • May employ a body chart • Identify areas and types of symptoms • Initial determination of the relationship between the symptomatic areas • What are included in the body chart? • Area • Constancy • Quality and severity • Relationship of the symptoms • Depth
Area and Type of Symptoms:Area • Provides information regarding: • Source of the problem • Prognosis • Used as baseline measure when monitoring treatment effects
Area and Type of Symptoms:Anesthesia/Paresthesia • Paresthesia vs. anesthesia • Paresthesia: altered sensation in an area • Anesthesia: absence of sensation (numbness) • Presence of altered sensation is suggestive of nerve compromise, particularly if the symptom distribution is dermatomal (Helfelt and Greubel 1978) • Most common cause of altered sensation accompanying spinal disorders is spinal/ nerve root compromise (Bogduk 1991)
Area and Type of Symptoms:Constancy • Are the symptoms present continuously? • Does the intensity of symptoms vary with movement or positioning? • Pain or paresthesia that is better or worse with movement or positioning is likely to be musculoskeletal in origin • Provides information regarding prognosis • Pain on activity that decreases with rest • Pain or aching as the day progress • Resting pain/ pain that is worse at the beginning of the activity • Intractable pain • Intermittent claudication • IV disc pain vs. facet pain
Area and Type of Symptoms:Quality • Refers to the description of pain • Interprets pain based on the pathology or structures involved • Indicates the severity of the pain experience • As part of a disability questionnaire • Throbbing diffuse – vasculature/ inflammation • Cramping dull aching – muscle • Sharp shooting – nerve • Deep nagging dull – bone • Sharp severe intolerable – fracture
Area and Type of Symptoms:Intensity • Rating severity of the symptoms based on a scale • Usually range from 0 (no pain) to 5/10 (severe pain) • Visual Analogue Scale: a 10-cm line with pain descriptors at each end (“no pain” to “pain as bad as it could be”) • May assist in determining prognosis • May be a reliable indicator of progress as the patient is providing information regarding the pain experience
Area and Type of Symptoms:Depth • It was previously believed that the depth of pain is related to the depth of injury. • Invalid considering spinal nerve or nerve root involvement • Imperative to have a good background knowledge of distribution/referral patterns for anatomical structures • Muscle pain does not refer superficially • Skin rarely refers pain • Visceral pain has cutaneous distribution/pattern and sometimes produce autonomic symptoms • Joints specifically zygapophyseal joint pain refer symptoms superficially
Area and Type of Symptoms:Relationship of Symptoms • Evaluate if the symptoms arise from one source or multiple sources • Identify whether symptoms are provoked independently (unrelated) or worsen all together (related) • Clinical Implication • Related symptoms: one area to be treated to relieve symptoms • Unrelated symptoms: a need to treat various areas to promote relief of symptoms
CURRENT HISTORY • History of the present illness • Provides information about the onset of the disorder • When the injury happened • Mechanism of injury (how the injury occurred) • Progress of symptoms • Treatment provided (if any) and effects of the treatment
Current History:Onset of Symptoms • Provides information of the relative stage of injury • Acute: 0 to 7 days after injury • Sub-acute: 7 days to 7 weeks after injury • Chronic: more than 7 weeks after injury • Allows the therapist to: • identify appropriate intervention • prognosticate • An insidious onset not related to injury or unusual activity is suspicious • Neoplasm • Degenerative lesions • Lesions due to tissue fatigue
Current History:Mechanism of Injury • Used to formulate diagnosis • Direction, position, and nature of the injuring force may provide clues which tissues could have been injured • Correlation can be made to the signs and symptoms for interpretation • The magnitude of the injuring force and the severity of injury can be compared • Take note of unusual injury patterns as these could be a sign of an abnormal tissue status prior to injury
Current History:Progress of Symptoms • Inquire if the patient’s symptoms get better, worse, or essentially status quo and in what way/manner • Most musculoskeletal injuries get better over time primarily due to the normal healing process (~ 6 weeks) • Some disorders may actually get worse over time underlying pathology • Pain that radiates: extends to include other areas • Presence of paresthesia following initial pain • Prognosis is good is the patient’s symptoms are improving
Current History:Treatment received and effects • If the patient has already been treated for the same injury in the past, or has received treatment prior to physical therapy consult, it is important to inquire about the type of intervention provided and the effects • Are noted changes for the better/worse? • Provides information regarding: • Prognosis • Treatment selection • Dosage of treatment
24-HOUR BEHAVIOR • Status of symptoms • At night • In the morning • Throughout the day: do the symptoms vary? • Knowledge of the behavior of the symptoms provides information in: • Formulation of diagnosis • Identifying plan of care • Monitoring of the progress of condition • Prognosis but only to a lesser extent
24-Hour Behavior:Night Pain • Does the patient have any difficulty sleeping because of the symptoms? • Does the pain wake the patient during sleep? • Probe deeper as to the quality of pain that cause such disturbance in sleep pattern • Determine worst and best sleeping positions • Incorporated in the patient care plan as interventions should increase patient’s comfort and ability to sleep Night time symptoms • Intractable pain – serious pathology • Unremitting pain – inflammatory pathology • Night time pain – muscle tears
24-Hour Behavior:Morning Pain • Provides information on how condition responds to rest • Identify the course of the symptom throughout the day • Musculoskeletal conditions respond well to rest • Stiffness, if present, resolve quickly especially with warm shower • Morning pain lasting more than 30 minutes is a sign of inflammatory arthritis
AGGRAVATING/ALLEVIATING FACTORS • What activities/positions aggravate/relieve the symptoms? • Knowledge of these may help in the diagnosis (identifies presence or absence of a mechanical problem), plan for physical examination, and the formulation of management • Pain aggravated by activity or relieved by rest can be suspected to arise from a pathologic process except in the case of a disk problem that is aggravated by sitting and relieved by walking and standing up • Arthritic conditions cause pain on the weight-bearing joints • Early stage: pain with prolonged walking or maintenance of weight-bearing • Late stage: pain prior to start of movement/walk that decreases while walking then returns after prolonged walking
IRRITABILITY • The ease with which a condition is exacerbated by movement • Three key questions to ask in order to determine the irritability of a condition: • What activity (and how much) aggravates symptoms? • How severe is the pain? • After cessation of the activity, how long till the pain returns to resting level? • What irritability of a condition provide the therapist? • How many and what active movements to examine • How far through the range of movement should the examination be performed • Which examination procedures to perform
PAST HISTORY • Previous episodes of the same condition will provide the therapist guidelines for: • Prognosis: duration and features may be similar to the previous condition • Treatment: identify which techniques are effective or not; additional intervention may be needed to prevent recurrence of the condition (if contributing factors have been well-established) • Diagnosis • Patient may have a different condition in the past that may have predisposed him/her to the current condition
PAST MEDICAL HISTORY • State of general health • Recent unexplained weight loss • Presence of osteoporosis • Cord signs • Dizziness • Headache • Other joints • Operations • Renal dialysis Provide precautions or contraindications to various treatment strategies
FAMILY HISTORY • Note disease process that have a familial incidence • Tumors • Heart disease • Arthritis • Allergies • Diabetes • Family history predisposes a patient to increased risk for acquiring the same condition
PERSONAL SOCIAL HISTORY • Social History • Employment status and requirements • Domestic role • No. of dependents • Recreational activities • Living conditions • Lifestyle
MEDICATIONS • Identify what medications the patient is taking, indication, dosage • Analgesics • Steroid intake • Maintenance medications • Side effects of the medications should be considered as these may interfere with the treatment
ANCILLARY PROCEDURES • Either rule out or confirm the presence of a condition that result to the patient’s symptoms • Laboratory and diagnostic test performed • Review of available records • Review of other clinical findings
CHIEF COMPLAINT andPATIENT’S GOALS • Usually stated as the problem that bothers them the most • Can be written verbatim: patient’s own words • Patient’s goal/s • Is it realistic? Is it achievable? • Allows the patient to have an active role in the planning of the treatment program
Objective Assessment • Facilitate or confirm the interpretation of subjective findings • Quantification of objective data allows documentation the patient’s baseline level of function or status accurate assessment of patient’s progress following a series of treatment sessions • Test and measures vary depending on the following: • Area to be examined • Information obtained from the subjective assessment
Objective Assessment • Ocular Inspection • Palpation • Range of Motion • Joint play • Muscle Performance/Motor control • Posture • Special Tests • Anthropometric measurements • Gait, locomotion, and balance • Functional assessment • Environmental assessment
Manner of arrival Ambulatory: independent or with device or dependent on caregiver for mobility Facial expression: apprehensive, restless, depressed, in discomfort Body type Ectomorph, endomorph, mesomorph Level of consciousness Attachments: cast, fixation devices, dressings Swelling Trophic skin changes Atrophy Gross deformities OCULAR INSPECTION
PALPATION The therapist should take note of the following: • Tenderness • Swelling • Variations in temperature • Muscle spasm • Differences in tissue texture • Abnormal sensation Grading of tenderness Grade I: pt complains of pain Grade II: pt complains of pain and winces Grade III: pt winces and withdraws the part Grade IV: pt does not allow palpation Swelling Bony/hard: osteophyte formation Boggy, spongy: synovial Soft, pliable, fluctuating: fluid Hard, thick, gel-like, warm: blood Thick, non-fluctuating, warm:pus Tough, dry, leathery:callus Thick, slow moving, indentation after pressure: pitting edema Abnormal Sensation Dysesthesia: diminished sensation Hyperesthesia: increased sensation Anesthesia: absence of sensation Crepitus: grating, creaking upon movement of a limb usually in the joint or tendinous unit
RANGE OF MOTION ASSESSMENT • Ask the patient to perform the painful movement as a baseline for your assessment • Observe / palpate the movement of the other joints • Watch out for trick movements • Check the end-feel
Range of Motion:Active ROM The therapist should note the following: • When and where during the movement onset of pain occurs • Whether the movement increases the quality of pain • Patient reaction • Amount of restriction and its nature • Pattern of movement • Quality of movement • Movement of associated joints • Willingness of the patient to move the segment
Range of Motion:Passive ROM The therapist should note the following: • When and where during movement the pain begins • Whether the movement increases the intensity and quality of pain • Pattern of limitation of movement • Capsular or non-capsular • End feel of movement • Movement of associated joints • Range of motion available
JOINT PLAY ASSESSMENT • Joint play refers to the small amount of ROM that can be obtained passively: ~4mm • The therapist should take into consideration the following: • Patient should be relaxed and fully supported • Use firm and comfortable grasp • Examine one joint and movement at a time • Test the unaffected side first • As one surface is moved, the other is stabilized • Movements should not be forced • Movements should not cause discomfort
MUSCLE PERFORMANCE • The therapist should assess various components of muscle performance (if appropriate): • Strength • Muscular endurance • Power • Agility • Use of manual muscle test (MMT), functional muscle test, fitness testing tools to determine baseline function of individual muscles or groups of muscles • When testing postural muscles, instead of using standard MMT, use motor control assessment
POSTURE • Provides information as to the probable cause of the deformity • The therapist should note the following: • Difference in alignment of the body segments: asymmetry • Presence of upper/lower crossed syndromes • Guidelines: • Patient appropriately undressed • No shoes, socks, stockings • Note use of walking aids, braces, etc. • Examine in the habitual, relaxed posture • Assess in standing, sitting, and lying positions Weak lengthened phasic muscles Tight hypertonic postural muscle JOINT Weak lengthened phasic muscles Tight hypertonic postural muscle
SPECIAL TESTS • Allows the therapist to: • Confirm a tentative diagnosis • Make a differential diagnosis • Differentiate between structures • Understand unusual signs • Unravel difficult signs and symptoms • Some tests have poor reliability and validity therefore the therapist should use these with caution • Findings depend on the skill and ability of the examiner to perform and identify (+) and (-) signs
ANTHROPOMETRIC MEASUREMENTS • Helps in formulation of a diagnosis/impression regarding the patient’s condition (leg length discrepancy), in prognosis (swelling), and in identifying the patient’s body type (skinfold measurement) • Performed in the presence of: • Swelling • Asymmetry in limb girth • Postural and gait deviations • Amputation
GAIT, LOCOMOTION ASSESSMENT • Majority of gait assessment is observation • The therapist should take note of the following: • Presence of gait deviations: abnormal gait patterns • Difference between the right and left lower extremity during specific cycles/phases of gait • Compensatory mechanisms • Speed and cadence of walking • Guidelines: • The patient should be assessed both in normal footwear and in bare feet • Take time to observe the patient during gait assessment • Assess in the anterior, posterior and lateral views • Note use of gait aids, etc.
FUNCTIONAL ASSESSMENT • Uses of functional assessment: • Helps the therapist establish what is important to the patient and the patient’s expectations • Represents a measurement of a whole-body task performance ability • Determines the effect of injury to the patient’s daily functions/activities • May involve task analysis, use of various functional assessment tools, fitness profiles
ENVIRONMENTAL ASSESSMENT • Home or workplace assessment provides the therapist information regarding the influence of the patient’s environment to the present condition • Are there any barriers to normal movement that predispose the patient to certain conditions? • Are modifications necessary to allow proper performance of activities?