Ankle osteoarthritis
270 likes | 480 Views
Ankle osteoarthritis. Dr F Pato May 2011. Patient case. 01-03-2011 69yr African female painful and swollen right ankle 2yrs Associated with swelling of feet at times. Difficulty in sleep O ccasional paraesthesia Tiredness R adiates to the hip joint.

Ankle osteoarthritis
E N D
Presentation Transcript
Ankle osteoarthritis Dr F Pato May 2011
Patient case • 01-03-2011 • 69yr African female • painful and swollen right ankle • 2yrs • Associated with swelling of feet at times. • Difficulty in sleep • Occasional paraesthesia • Tiredness • Radiates to the hip joint.
Walks with aid (easy mobilization and balance) • limping gait • Weight transferred to the left side of the body. • She has been seen with this complaint by GP. • Patient is also having bilateral flank pain.
Prev medical history: hypertension, rheumatoid arthritis, dermatitis • Prev surgical history: sterilisation • Medication: antihypertensive • Allergies: Unknown • Family history: Hypertension • Social: Pensioner, non-smoking, non-alcohol user, lives with grandchildren en looks after them.
On Examination • Overweight • Oedema of the ankles and knees • Cardiovascular: intact • Respiratory: intact • Abdomen: central obesity • Skin: Dermatitis
Examination cont • Ankle joint: • Range of movement decreased in all directions. • Passive and active • Pain with inversion of right ankle • Rest of movement not painful, active en passive. • No notable deformities from rheumatoid arthritis.
Assessment • 3point assessment: • Subjective: Pain hinders with the level of daily function, that is: playing with the children and taking care of the house and yard. She wants pain relief • Objective: Rheumatoid arthritis of ankle and knee joints, osteoarthritis • Contextual: osteoarthritis secondary to rheumatoid arthritis and obesity. • Assessment: rheumatoid arthritis, osteoarthritis, obesity, urinary tract infection.
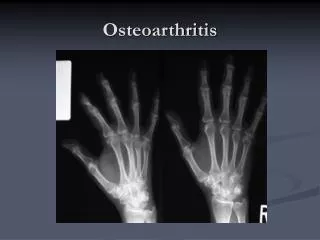
Plan: urine dipstix, x-ray • X-ray: decreased joint space and osteophyte formation at the margin plus bone cysts. No signs of previous injury. • Advise exercise and weight reduction to relieve pressure applied to the joints • Exercises prescribed: walking, squats, dorsiflexion, eversion and inversion, heel raisers. Help with strengthening of the muscles around the joints and maintainance of movement.
Review 28.03.2011 • Range of movement better. • Pain improving. Swelling less. • On examination: Swelling subsided. • Still walking with aid • Less antalgic. • Range of movement improved. • Patient to continue with exercise at home. Review in 1 month.
Osteoarthritis • Definition • Rheumatological condition • Synovial inflammatory response • Imbalance in joint tissue breakdown and repair 3 • Subchondral bone sclerosis • Erosion of articular cartilage • Deposition of osteophytes • Structural and functional failure of synovial joints3
Epidemiology • 6% above 30yrs (2006), 13% >60 (1998) • Depends on method used to classify • Radiographs or self report • Risk factors • Age, gender, diet, family history, obesity, joint injury, endocrine, occupational
Anatomy • Bones Tibia Fibula Talus
Ligaments • Ligamnets • Lateral • Ant talofibular • Post talofibular • Calcaneofibular • Medial • Ant tibiotalar • Tibionavicular • Tibiocalcaneal • Post tibial part
Management methods Weight reduction not costly reduces joint load Compliance with diet Not guaranteed to help Exercise increases mobility Symptomatic relief only
Management methodscont NSAIDS Reduce pain and inflammation Side effects ? chondrodestructive Simple analgesia Safe, cheap, relieve mechanical pain Often incomplete control of symptoms Osteotomy Relieves painful movement Increases joint mobility Limited success rate
Management methods cont Arthroplasty Relieves painful movement Increases joint mobility Cost Prosthesis lifespan and failure Intra articular steroids Temporary decrease in stiffness and inflammantion May cause joint degradation side effects
Exercise and articular cartilage • Exercise prescription3 • Weight loss • Joint range of motion preserved • Functional performance improvement • Strength improvement • Symptom reduction • Start with isometric then move to isotonic resistance as tolerated • Promotion of low-impact exercise • Encourages exercise benefits • Avoids potential damaging effects of high-impact activities
Literature cont • FavourabledGEMRIC index • (Delayed Gadolinium Enhanced MRI of cartilage) • Compared sedentary vs exercise intervention • Increased proteoglycan • Cross sectional study (2004) • OA risk increased by activity of high impact and high stress to the joint, increased by the presence of previous injury to the specific joint • Overexercise leads to glycosaminoglycan depletion • Lack of mechanical stimulation leads to cratilage atrophy • ? cartilage transplants
Literature cont • Human cartilage recovers within 90 min after loading • Appeared to deform a little in the 1st few minutes under high loads • Very little deformation shown • Increased loading not associated with articular thickening • Deformation is dependent on biochemical composition of tissue • Aid in designing of artificial cartilage
Literature cont • Deformation difficult to assess during loading • Age results in linear decrease in cartilage thickness with or without OA • Cartilage thickness is genetically determined • Different genes responsible for different joints • Study comparing siblings and twins Prevention of further degradation and maintaining functionality of joint is important
References • Clinical sports medicine revised third edition, P Brukner, K Khan • Clinically orientated anatomy fourth edition. K I Moore and A F Dalley • David J. Hunter. Felix Eckstein. Exercise and osteoarthritis, Journal of Anatomy2009.214(2):197-207 • Lecture notes, D Whitelaw, osteoarthritis lecture notes, 2005 • F. Eckstein, M. Huldelmaier, R. Putz. Effects of exercise on human articular cartilage, Journal of Anatomy2006.208:491-512