Download

1 / 26
840 likes | 1.59k Views
Osteoarthritis. OA is uncommon in adults under age 40 and highly prevalent in those over age 60 In middle-aged and elderly persons, is much more common in women than in men, Obesity, a major risk factor Commonly affected joints cervical and lumbosacral spine, hip, knee, and

E N D
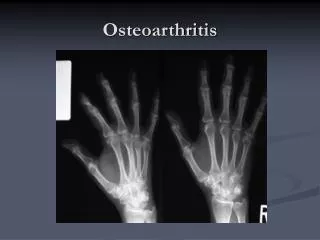
OA is uncommon in adults under age 40 and highly prevalent in those over age 60 • In middle-aged and elderly persons, is much more common in women than in men, • Obesity, a major risk factor • Commonly affected joints cervical and lumbosacral spine, hip, knee, and first metatarsal phalangeal joint (MTP). In the hands, the distal and proximal interphalangeal joints and the base of the thumb are often affected
Definition OA is joint failure, a disease in which all structures of the joint have undergone pathologic change, often in concert Joint Protective Mechanisms and Their Failure Joint capsule and ligaments serve as joint protectors by providing a limit to excursion, thereby fixing the range of joint motion. Synovial fluid reduces friction between articulating cartilage surfaces, thereby serving as a major protector against friction-induced cartilage wear. lubricin, a mucinous glycoprotein secreted by synovial fibroblasts whose concentration diminishes after joint injury and in the face of synovial inflammation The ligaments, along with overlying skin and tendons, contain mechanoreceptor sensory afferent nerves mechanoreceptors -assume the right tension at appropriate points in joint excursion to act as optimal joint protectors, anticipating joint loading
Muscles and tendons that bridge the joint are key joint protectors Failure of these joint protectors increases the risk of joint injury and OA. Cartilage and Its Role in Joint Failure The two major macromolecules in cartilage are type 2 collagen, and Aggrecan In normal cartilage, type 2 collagen is woven tightly, constraining the aggrecan molecules in the interstices between collagen strands, forcing these highly negatively charged molecules into close proximity with one another The aggrecan molecule, through electrostatic repulsion of its negative charges, gives cartilage its compressive stiffness
Chondrocytes,-- synthesize all elements of the matrix. - produce enzymes that break down the matrix and cytokines and growth factors, Cartilage matrix synthesis and catabolism are in a dynamic equilibrium influenced by the cytokine and growth factor environment. Mechanical and osmotic stress on chondrocytes induces these cells to alter gene expression and increase production of inflammatory cytokines and matrix-degrading enzymes. Type 2 cartilage is degraded primarily by MMP-13 (collagenase 3) Aggrecan degradation - activation of two aggrecanases (ADAMTS-4 and ADAMTS-5) and perhaps of MMPs. Both collagenase and aggrecanases act primarily in the territorial matrix surrounding chondrocytes; however, as the osteoarthritic process develops, their activities and effects spread throughout the matrix, especially in the superficial layers of cartilage.
Interleukin (IL) 1, which exerts transcriptional effects on chondrocytes, stimulating production of proteinases and suppressing cartilage matrix synthesis Tumor necrosis factor (TNF) may play a similar role to that of IL-1 These cytokines also induce chondrocytes to synthesize prostaglandin E2, nitric oxide, and bone morphogenic protein 2 (BMP-2), which together have complex effects on matrix synthesis and degradation Nitric oxide inhibits aggrecan synthesis and enhances proteinase activity, whereas BMP-2 stimulates anabolic activity At early stages in the matrix response to injury and in the healthy response to loading, the net effect of cytokine stimulation may be matrix synthesis but, ultimately, excess IL-1 triggers matrix degradation. OA cartilage is characterized by gradual depletion of aggrecan, an unfurling of the tightly woven collagen matrix, and loss of type 2 collagen
Systemic Risk Factors Age is the most potent risk factor for OA. dynamic loading of joints stimulates cartilage matrix synthesis by chondrocytes in young cartilage, aged cartilage is less responsive to these stimuli. Muscles that bridge the joint become weaker with age and also respond less quickly to oncoming impulses. Sensory nerve input slows with age, retarding the feedback loop of mechanoreceptors to muscles and tendons related to their tension and position. Ligaments stretch with age, making them less able to absorb impulses. These factors work in concert to increase the vulnerability of older joints to OA. Older women are at high risk of OA in all joints
Heritability and Genetics the heritable proportion of knee OA is at most 30%, genetic mutations that confer a high risk of OA, one of which is a polymorphism within the growth differentiation factor 5 gene. Risk Factors in the Joint Environment developmental abnormalities occurring in utero or childhood, congenital dysplasia, Legg-Perthes disease, and slipped capital femoral epiphysis, leave a child with distortions of hip joint anatomy that often lead to OA later in life. fracture through the joint surface often causes OA in joints in which the disease is otherwise rare such as the ankle and the wrist. Avascular necrosis can lead to collapse of dead bone at the articular surface, producing anatomic irregularities and subsequent OA Tears of ligamentous and fibrocartilaginous structures that protect the joints, such as the anterior cruciate ligament and the meniscus in the knee and the labrum in the hip, increase joint susceptibility and can lead to premature OA
Risk factors for osteoarthritis include the following : Age Obesity (increases mechanical stress) Trauma Genetics Sex hormones Muscle weakness Repetitive use (ie, jobs requiring heavy labor and bending) Infection Crystal deposition Acromegaly Previous rheumatoid arthritis (ie, burnt-out rheumatoid arthritis) Heritable metabolic causes (eg, alkaptonuria, hemochromatosis, Wilson disease) Hemoglobinopathies (eg, sickle cell disease, thalassemia) Neuropathic disorder leading to a Charcot joint (eg, syringomyelia, tabes dorsalis, diabetes) Underlying orthopedic disorders (eg, congenital hip dislocation, slipped femoral capital epiphysis) Disorders of bone (eg, Paget disease, avascular necrosis
men with a history of major knee injury, but no surgery, had a 3.5-fold increased risk for subsequent knee OA. malalignment across the joint
Loading Factors Obesity Repeated Use of Joint farmers are at high risk for hip OA, and miners have high rates of OA in knees and spine textile mill, women whose jobs required fine pincer grip [increasing the stress across the interphalangeal (IP) joints] had much more distal IP (DIP) joint OA
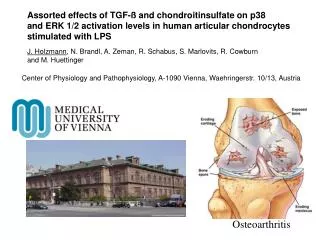
Pathology Cartilage surface fibrillation and irregularity focal erosions extend down to the subjacent bone. cartilage erosion expands to involve a larger proportion of the joint surface loss of cartilage come alterations in subchondral bone At the margin of the joint, near areas of cartilage loss, osteophytes form capsule, which stretches, becomes edematous, and can become fibrotic
Pain mechanisms in osteoarthritis Pain, the main presenting symptom of osteoarthritis, is presumed to arise from a combination of mechanisms, including the following: Osteophytic periosteal elevation Vascular congestion of subchondral bone, leading to increased intraosseous pressure Synovitis with activation of synovial membrane nociceptors Fatigue in muscles that cross the joint Overall joint contracture Joint effusion and stretching of the joint capsule Torn menisci Inflammation of periarticular bursae Periarticular muscle spasm Psychological factors Crepitus (a rough or crunchy sensation)
Clinical Features Pain comes on either during or just after joint use In knees, buckling may occur, in part, due to weakness of muscles crossing the joint tenderness is over the joint line
Diagnostic Considerations The initial goal is to differentiate osteoarthritis from other arthritides, such as rheumatoid arthritis. Rheumatoid arthritis . Additional arthritides Clinical history and characteristic radiographic findings can be used to differentiate spondyloarthropathy from sacroiliac and lumbosacral spine involvement. Secondary osteoarthritis must be considered in individuals with chondrocalcinosis, joint trauma, metabolic bone disorders, hypermobility syndromes, and neuropathic diseases. The elbow is not commonly affected in osteoarthritis; however, elbow arthritis Osteoarthritis of the elbow is not commonly seen; however, it can occur with a history of previous trauma.
The following should also be considered in the differential diagnosis: Crystal deposition disease Pseudogout Inflammatory arthritis Seronegative spondyloarthropathies Infected joint Underlying mechanical pain Reactive arthritis Examination of the synovial fluid is often more helpful diagnostically than an x-ray. If the synovial fluid white count is >1000 per L, inflammatory arthritis or gout or pseudogout are likely, the latter two being also identified by the presence of crystals.
Treatment: Osteoarthritis Nonpharmacotherapy • avoiding activities that overload the joint, as evidenced by their causing pain; (2) improving the strength and conditioning of muscles that bridge the joint, so as to optimize their function; and (3) unloading the joint, either by redistributing load within the joint with a brace or a splint or by unloading the joint during weight bearing with a cane or a crutch. Exercise Correction of Malalignment
Pharmacotherapy Surgery