Download
1 / 15
150 likes | 819 Views
Bacteremia and Endocarditis: Products and Guidance. Janice Soreth, MD Director Division of Anti-Infective and Ophthalmology Products. PDR Search: Products Labeled for Endocarditis/Bacteremia. Imipenem Cefazolin Gentamicin Vancomycin Nafcillin Oxacillin. Imipenem.

E N D
Bacteremia and Endocarditis: Products and Guidance Janice Soreth, MD Director Division of Anti-Infective and Ophthalmology Products
PDR Search: Products Labeled for Endocarditis/Bacteremia • Imipenem • Cefazolin • Gentamicin • Vancomycin • Nafcillin • Oxacillin
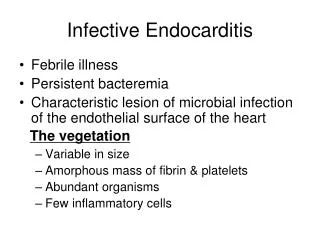
Imipenem • Bacterial septicemia. Enterococcus faecalis, Staphylococcus aureus (penicillinase-producing strains), Enterobacter species, Escherichia coli, Klebsiella species, Pseudomonas aeruginosa, Serratia species,Bacteroides species including B. fragilis • Endocarditis. Staphylococcus aureus (penicillinase-producing strains)
Cefazolin • Septicemia: Due to S. pneumoniae, S. aureus, P. mirabilis, E. coli. • Endocarditis: Due to S. aureus (including (beta)-lactamase-producing strains) and S. pyogenes .
Vancomycin • Vancomycin is indicated for the treatment of serious or severe infectionscaused by susceptible strains of methicillin-resistant (beta-lactam-resistant) staphylococci. It is indicated for penicillin-allergic patients, for patients who cannot receive or who have failed to respond to other drugs, including the penicillins or cephalosporins, and for infections caused by vancomycin-susceptible organisms that are resistant to other antimicrobial drugs. Vancomycin is indicated for initial therapy when methicillin-resistant staphylococci are suspected, but after susceptibility data are available, therapy should be adjusted accordingly. • Vancomycin is effective in the treatment of staphylococcal endocarditis. • Its effectiveness has been documented in other infections due to staphylococci, including septicemia, bone infections, lower respiratory tract infections, skin and skin structure infections. • When staphylococcal infections are localized and purulent, antibiotics are used as adjuncts to appropriate surgical measures.
Gentamicin • Gentamicin …has been found effective when used in conjunction with a penicillin-type drug for the treatment of endocarditis caused by group D streptococci. • Gentamicin has also been shown to be effective in the treatment of serious staphylococcal infections. While not the antibiotic of first choice, gentamicin may be considered when penicillins or other less potentially toxic drugs are contraindicated and bacterial susceptibility tests and clinical judgment indicate its use. • In the neonate with suspected bacterial sepsis or staphylococcal pneumonia, a penicillin-type drug is also usually indicated as concomitant therapy with gentamicin.
Nafcillin • Nafcillin is indicated in the treatment of infections caused by penicillinase-producing staphylococci which have demonstrated susceptibility to the drug. • Culture and susceptibility tests should be performed initially to determine the causative organism and its susceptibility to the drug. • Nafcillin may be used to initiate therapy in suspected cases of resistant staphylococcal infections prior to the availability of susceptibility test results. • Nafcillin should not be used in infections caused by organisms susceptible to penicillin G.
Design of Previous Studies for Bacteremia and Endocarditis Claims (pre-1990s) • Multicenter study of the comparative efficacy, safety, and tolerance of drug X and drug Y in the parenteral therapy of infections in hospitalized patients caused by susceptible pathogenic bacteria • Infections studied in one trial included lower respiratory, skin, gynecologic, UTI, bone and joint, septicemia, and endocarditis, with treatment duration ranging from a week to a month or longer • Experience in bacteremia or endocarditis usually in a “handful”, sometimes supplemented with case series or data from uncontrolled study
1992 Points to Consider Document: Endocarditis • One open trial of at least 50 patients that establishes a predetermined overall clinical and microbiologic success rates is suggested. • If there is not a reasonable mix of artificial and native valve, right and left sided disease, and acute versus subacute clinical presentations, such should be noted in the approved labeling by restricting the labeling in the INDICATIONS AND USAGE section of the product labeling to just those types of infection and populations actually studied. • This trial should involve at least two investigators in different geographic areas. Pathogens listed would be determined on a case-by-case basis, taking into account various expected success rates for the treatment of specific pathogens.
Anti-infectives approved for endocarditis post 1992 Guidance This slide is intentionally blank.
2004 AIDAC Recommendations to FDAon S. aureus bacteremia indication • Re-write the draft guidance on catheter related bloodstream infections to reflect the current reality of patient/public health needs and resources for drug development. • Balance good science with practicalities of clinical trial design and conduct. • Study patients with S. aureus bacteremia, including in a development program patients with defined sites of infection and concurrent bacteremia, as well as those without an identified organ site (“primary”).
The Study • Sponsor, Cubist Pharmaceuticals, designed and conducted a study in the treatment of patients with S. aureus bacteremia and endocarditis. • Sponsor and FDA agreed upon the study design: a randomized, open-label, controlled trial of daptomycin versus standard of care in a group of patients who have S. aureus in the blood, some of whom have endocarditis • The study echos what physicians face: the management of patients with staphylococcal bacteremia, including patients with endocarditis.
Today’s Agenda • Overview • Clinical Trial (Sponsor and FDA talks) • Charge to the Committee
Critical Path Initiative An attempt to bring attention and focus to the need for targeted scientific efforts, to address unmet medical need, and to improve the techniques and methods used to evaluate the safety, efficacy and quality of medical products as they move from product selection, design, mass manufacture, and use.