Prescribing Controlled Substances Responsibly
130 likes | 305 Views
Prescribing Controlled Substances Responsibly. Lianne Beck, MD Assistant Professor Emory Family Medicine. Scope of the Problem.

Prescribing Controlled Substances Responsibly
E N D
Presentation Transcript
Prescribing Controlled Substances Responsibly Lianne Beck, MD Assistant Professor Emory Family Medicine
Scope of the Problem • In 2005, more than 10 million Americans were abusing prescription drugs – more than the combined number of people abusing cocaine, heroin, hallucinogens and inhalents. • The CDC report that prescription opioids are now associated with more drug overdose deaths than cocaine and heroin combined: between 1999 and 2002 there was a 91% increase in the reporting of opioid analgesics on death certificates.
Scope of the Problem • In 2005, more new drug users began abusing pain relievers (2.2 million) than marijuana (2.1 million) or cocaine (872,000). By comparison, in 1990 only an estimated 628,000 people initiated illicit use of pain killers. • Data from a set of selected states show that almost 13,000 incidents of prescription controlled substances were diverted by theft from 2000 to 2003. In 2003 alone, 2 million dosages of six opioid analgesics were reported stolen from the supply chain, mainly from retail pharmacies.
Scope of the Problem • http://www.ajc.com/news/gwinnett/prescription-drugs-popular-among-372523.html • http://www.gcpstv.org/
Drug Schedules • http://www.mspta.com/dre/pdf/Drug%20schedules.pdf
Drug Seeking Behaviors • Unusual behavior in the waiting room. • Assertive personality, often demanding immediate action. • Unusual appearance - extremes of either slovenliness or being over-dressed. • May show unusual knowledge of controlled substances and/or gives medical history with textbook symptoms OR gives evasive or vague answers to questions regarding medical history. • Reluctant or unwilling to provide reference information. Usually has no regular doctor and often no health insurance.
Drug Seeking Behaviors • Will often request a specific controlled drug and is reluctant to try a different drug. • Generally has no interest in diagnosis - fails to keep appointments for further diagnostic tests or refuses to see another practitioner for consultation. • May exaggerate medical problems and/or simulate symptoms. • May exhibit mood disturbances, suicidal thoughts, lack of impulse control, thought disorders, and/or sexual dysfunction. • Cutaneous signs of drug abuse - skin tracks and related scars on the neck, axilla, forearm, wrist, foot and ankle. Such marks are usually multiple, hyper-pigmented and linear. New lesions may be inflamed. Shows signs of "pop" scars from subcutaneous injections.
Drug Seeking Behaviors • Must be seen right away. • Wants an appointment toward end of office hours. • Calls or comes in after regular hours. • States he/she's traveling through town, visiting friends or relatives (not a permanent resident). • Feigns physical problems, such as abdominal or back pain, kidney stone, or migraine headache in an effort to obtain narcotic drugs. • Feigns psychological problems, such as anxiety, insomnia, fatigue or depression in an effort to obtain stimulants or depressants.
Drug Seeking Behaviors • States that specific non-narcotic analgesics do not work or that he/she is allergic to them. • Contends to be a patient of a practitioner who is currently unavailable or will not give the name of a primary or reference physician. • States that a prescription has been lost or stolen and needs replacing. • Deceives the practitioner, such as by requesting refills more often than originally prescribed. • Pressures the practitioner by eliciting sympathy or guilt or by direct threats. • Utilizes a child or an elderly person when seeking methylphenidate or pain medication.
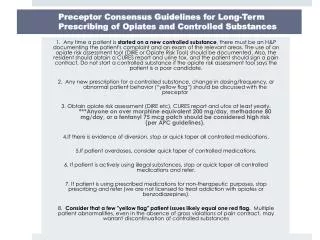
Federation of State Medical BoardsModel Policy • Patient evaluation, including risk assessment • Treatment plans that incorporate functional goals • Informed consent and prescribing agreements • Periodic review and monitoring of patients • Referral and patient management • Documentation • Compliance with state and federal law
Functional Goals Evidence • Begin physical therapy • Sleep in a bed as opposed to a lounge chair • Participation in a pain support group • Increase activities of daily living • Walk around the block • Increased social activities • Resumed sexual relations • Returned to work • Daily exercise • Letter from physical therapist • Report by family member or friend • Letter from group leader • Report by family member or friend • Pedometer recordings or written log of activity • Report by family member/friend • Report by partner • Pay stubs or letter from employer • Gym attendance records or report from family member/friend
Helpful Resources • Tips for Georgia Physicians • http://gdna.georgia.gov/00/channel_modifieddate/0,2096,132319894_145437852,00.html • Guidelines for Use of Controlled Substances for the Treatment of Pain: Ten Steps • http://dps.georgia.gov/vgn/images/portal/cit_1210/45/23/36282207PAIN_MANAGEMENT_041008.pdf • http://www.fsmb.org/pain/ • http://www.painmed.org/pdf/noncancer_opioid_guidelines.pdf