Download

1 / 41
410 likes | 588 Views
High-throughput Clinical Cancer Genotyping A. John Iafrate , MD/PhD Department of Pathology Diagnostic Molecular Pathology Laboratory Translational Research Laboratory Massachusetts General Hospital Boston, MA aiafrate@partners.org. A New Paradigm in Cancer Treatment. Cancer Patient.

E N D
High-throughput Clinical Cancer Genotyping A. John Iafrate, MD/PhD Department of Pathology Diagnostic Molecular Pathology Laboratory Translational Research Laboratory Massachusetts General Hospital Boston, MA aiafrate@partners.org
A New Paradigm in Cancer Treatment Cancer Patient Clinical Information Targeted Therapy Surgical Resection Molecular Pathology Routine Pathology
A New Paradigm in Cancer Treatment Haber, Gray, Baselga Cell 2011
BRAF 1799 T>A V600E BCR-ABL Imatinib 100% CML HER2 Trastuzumab 20-30% IDC ALK Crizotinib 3-5% Lung adenocarcinoma EGFR Erlotinib/ Gefitinib 20% Lung adenocarcinomas BRAF V600E PLX4032 50-60% Melanoma
BRAF 1799 T>A V600E BCR-ABL Imatinib 100% CML HER2 Tastuzumab 20-30% IDC O’Brien et al., Imatinib Compared with Inter-feron and Low-Dose Cytarabine for Newly Diagnosed Chronic-Phase Chronic Myeloid Leukemia, NEJM 2003 ALK Crizotinib 3-5% Lung adenocarcinoma EGFR Erlotinib/ Gefitinib 20% Lung adenocarcinomas BRAF V600E PLX4032 60% Melanoma Romond EH et al., Trastuzumab plus Adjuvant Chemotherapy for Operable HER2-Positive Breast Cancer. NEJM 2005. Mok et al., NEJM 2009
Comprehensive Genetic Characterization of Tumors for Personalized Cancer Care DNA epigenetics DNA mutations DNA chromosomal alterations Proteomics mRNA and miRNA profiling
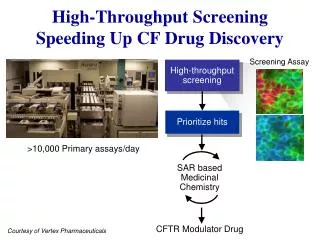
Clinical Genotyping in Guiding Therapeutic Decisions • Real-time screening of patient tumor samples for genetic alterations. • Employing high-throughput genotyping technologies. • (>100 samples/week) • Directing patient therapy based on genetic fingerprint. Cancer Patients Prospective Enrollment Oncology Clinical trials Genotyping Improved Clinical Use of Genotyping MGH Translational Research Laboratory MGH Pathology Specimen Repository Basic Research Centers
Challenges in Establishing a Clinical Genotyping Program • Platform and clinical validation • Archived specimen size and quality • Informatics • Turn-around time • Disease group customer support • Phased roll-out • Lung, Colon, GBM, Breast • Finances and billing
ddNTP ddNTP ddNTP loci of interest Relative fluorescence Increasing molecular weight A B C D E F SNAPSHOT Overview Multiplex PCR Single Base Extension Reaction Capillary Electrophoresis Electrophoretic Output
SNAPSHOT Genotyping Assay 16 cancer genes – 120 described mutations AKT1 49G – E17 ERBB2 Exon 20 insertions IDH1 R132 -394C IDH1 R132 -395G
bCat121 EGFR2235_49F bCat94 PI3K1633 Panel 1 7-plex KRAS34 EGFR 2573 NRAS181 NRAS38 bCat122 PI3K263 8-plex Panel 2 NRAS182 bCat95 BRAF1799 EGFR2235_49R TP53.742 EGFR2369 5-plex Panel 3 EGFR2236_50F PI3K1624 NRAS35 bcat133 PTEN517 KRAS35 8-plex Panel 4 FLT3.2503 NOTCH1.4724 EGFR2236_50R PI3K3139 NOTCH1.4802 TP53.733 SNAPSHOT v3
SNAPSHOT v3 Normal Lung cancer EGFR mutation Glu746_Ala750del (c.2235_2249del)
SNAPSHOT v3 Normal Melanoma BRAF mutation Val600Glu (c.1799T>A)
SNAPSHOT v3 Normal Colorectal cancer KRAS mutation Gly13Asp (c.38G>A)
SNAPSHOT v3 Normal Breast cancer PIK3CA mutation His1047Arg (c.3140A>G)
AKT 1% NRAS 1% BRAF 2% IDH1 <1% HER2 2% CTNNB1 2% ALK 3% PIK3CA 4% TP53 5% No Mutation 42% EGFR 15% KRAS 23% Mutational profiling in lung cancers N=650
Lung Adenocarcinoma: Overlap of Mutations KRAS 56 isolated (58 total) PIK3CA 5 EGFR 36 isolated (50 total) 1 1 B-cat 1 3 1 TP53 T790M 5 2 1 1 1 4 ALK 13 APC 2 BRAF 1 NRAS Belinda Waltman/ Lecia Sequist
Rapid integration of FISH : ALK Rearrangements in NSCLC Crizotinib: Potent & selective ATP competitive oral inhibitor of MET and ALK kinases and their oncogenic variants
Phase I Clinical Trial of ALK Inhibitor Crizotinib in ALK-rearranged Lung Adenocarcinoma
Timeline for Crizotinib and ALK in NSCLC PF2341066 activity in cells exhibiting ALK fusion in broad screen (MGH-McDermott) PF2341066 Inhibits ALK activity PF2341066 FIP May 2005 2006 2007 2008 2009 Objective responses demonstrated in ALK fusion positive NSCLC and IMT Identification of PF2341066 PF2341066 demonstrates cytocidal activity in cells exhibiting ALK fusion (Pfizer in house) Discovery of EML4-ALK fusions in NSCLC (CREST) Japan Science & Technology Agency) Phase III study of “Crizotinib” in ALK positive NSCLC starts Slide Courtesy of Ross Camidge
Timeline for Crizotinib and ALK in NSCLC For phase I trial: ALK enriched cohort of 82 subjects required FISH screening of over 1200 NSCLCs PF2341066 activity in cells exhibiting ALK fusion in broad screen (MGH-McDermott) PF2341066 Inhibits ALK activity PF2341066 FIP May 2005 2006 2007 2008 2009 Objective responses demonstrated in ALK fusion positive NSCLC and IMT Identification of PF2341066 PF2341066 demonstrates cytocidal activity in cells exhibiting ALK fusion (Pfizer in house) Discovery of EML4-ALK fusions in NSCLC (CREST) Japan Science & Technology Agency) Phase III study of “Crizotinib” in ALK positive NSCLC starts Slide Courtesy of Ross Camidge
Formation of Lung Cancer Mutation Consortium (LCMC) NIH-funded multicenter genotyping trial with mission of cross-validating platforms and accelerating recruitment into clinical trials of targeted agents. Close collaboration of oncologists, pathologists and molecular diagnosticians
APC 4% NRAS 3% No Mutation Identified 34% BRAF 7% PIK3CA 6% KRAS 25% TP53 21% Mutational profiling in colorectal cancers N=250
BRAF 6 isolated PIK3CA 3 KRAS 20 isolated (36 total) 3 TP53 18 isolated (28 total) 1 4 1 1 4 APC 1 2 6 NRAS 3 1 Colon Adenocarcinoma: Overlap of Mutations
Genomic TL-09-267 20 ng/panel DNA TL-09-285 3.04ng/panel DNA
The Future of Clinical Cancer Genotyping Do we have the technology? Is it cost-effective? What to genotype? The challenges? By Angela Canada Hopkins
Next Generation Sequencing Next Generation Sequencing First Generation Sequencing
Next Generation Sequencing Roche 454 Illumina/Solexa Life Technology SOLiD Helicos
Next Generation Sequencing • Illumina HiSeq 2000 • Up to 1 billion clusters • 150-200 Gb with 8 day run time • $690K, ~$10000 per human genome sequencing • 4 cameras, 50 MB/s of imaging, 4 x 625 MB images every 30 seconds 32 TB if raw images stored
Next Generation Sequencing Roche 454 GS Jr Illumina MiSeq Life Technology Ion Torrent
Cancer Driver Mutations Non-Silent Mutations in Pancreatic Cancer Bert Vogelstein: AACR 2010 Meeting Plenary Session Mutations per Tumor • Published Cancer Exomes • 11 Colorectal – Science 2007 • 11 Breast – Science 2007 • 24 Pancreas – Science 2008 • 22 Gliomas – Science 2008 • 2 Leukemias – NEJM, Nature 2008 • 1 Breast – Nature 2010 • 1 Breast – Nature 2009 • 4 Granulosa Cell – NEJM 2009 • 1 Lung – Nature 2010 • 1 Melanoma – Nature 2010 • 22 Medulloblastomas - Unpublished Non-Silent Mutations in Different Tumors Mutations per Tumor
Cancer Driver Mutations: How Many? Genetic Alterations in Pancreatic Cancer Bert Vogelstein: AACR 2010 Meeting Plenary Session Mutations per Tumor • Review of Literature/Databases • 116,432 human cancers • 353 histopathologic subtypes • 130,072 intragenic somatic mutations • 3142 mutated genes • Potential Driver Genes • 286 tumor suppressor genes (>15% of mutations are truncating) • 33 oncogenes (same codon mutated in at least 2 tumors) Driver Gene Alterations in Pancreatic Cancer Mutations per Tumor
Somatic Mutations: How much to sequence? • Desired Analytical Sensitivity • 1-5% • Typical NGS Error Rate • 1-2% • Whole Genome Sequencing • 30x • 1 error >3.3% sensitivity • Targeted Sequencing • 200-500x • 0-4 errors in 200 reads 1%-2% error • Set threshold at ≥5% • Whole Genome Sequencing at 200x • >$60,000!
Clinical Cancer Genotyping: On the Horizon • Clinical targeted sequencing of FFPE DNA • initially 100 exons >1000 • 200-500X coverage • 100-150+ Mb data • 3-4 week turnaround time • $500 raw reagent cost • Desired • Whole exon coverage • Tumor vs. normal? • Copy number? • Rearrangements? • Methylation? • Transcription?
Summary • Cancer genetics is rapidly expanding with high complexity • Molecular profiling will drive cancer management • Continued need for higher-throughput cancer genotyping • Clinical next generation sequencing is coming • Collaborative efforts such as genotyping consortium will be • key to addressing problem of cancers with rare genotypes
MGH Molecular Diagnostics Leif Ellisen Darrel Borger Dora Dias-Santagata Kathy Vernovsky Arjola Cosper Breton Roussel Kristin Bergethon Hannah Stubbs Vanessa Scialabba Sara Akhavanfard MGH Cancer Center Daniel Haber David Louis Eunice Kwak Jeff Clark Mari Mino-Kenudson Eugene Mark Jeff Engelman Ultan McDermott Jeff Settleman Lecia Sequist Belinda Waltman Alice Shaw COI Disclosure: AJI has a paid consulting relationship with Pfizer Inc. and has a provisional patent for SNaPshot assay.