Download
1 / 26
371 likes | 1.64k Views
Crossed-Fused Renal Ectopia imaged with Tc99m-MAG₃. Mike Durkan SPRING Term 2008-09 Nuclear Medicine Externship Case Study. TABLE OF CONTENTS. LIST OF FIGURES------------------------------------------------------------ 3

E N D
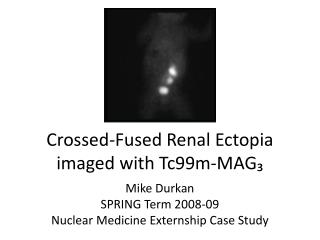
Crossed-Fused Renal Ectopia imaged with Tc99m-MAG₃ Mike Durkan SPRING Term 2008-09 Nuclear Medicine Externship Case Study
TABLE OF CONTENTS LIST OF FIGURES------------------------------------------------------------ 3 INTRODUCTION------------------------------------------------------------ 4 DYNAMIC MAG-3 RENOGRAM----------------------------------------- 5-10 CONGENITAL RENAL ABNORMALITES-------------------------------- 11-12 RENAL FUSION CLASSIFICATION---------------------------------------- 13 HORSESHOE KIDNEY ANATOMY----------------------------------------- 14 HORSESHOE KIDNEY VARIATIONS-------------------------------------- 15 ECTOPIC PELVIC KIDNEY--------------------------------------------------- 16 CROSSED-FUSED RENAL ECTOPIA--------------------------------------- 17 RENAL ECTOPIA EMBRYOLOGICAL ETIOLOGY------------------------ 18 PATIENT HISTORY------------------------------------------------------------ 19 IMAGE FINDINGS------------------------------------------------------------ 20 IMAGE FINDINGS: MAG₃ RENOGRAM---------------------------------- 21-22 CONCLUSION------------------------------------------------------------------ 23 REFERENCES------------------------------------------------------------------- 24-26
LIST OF FIGURES Fig. 1: Mag₃ Renogram 30 min image; [neonatal polycystic kidney]------------------------------------------- 5 Fig. 2: 20 ml emulsion ampoule of Propofol ------------------------------------------------------------------------ 6 Fig. 3: Renal Nephron cut-away---------------------------------------------------------------------------------------- 7 Fig. 4: Detector FOV------------------------------------------------------------------------------------------------------- 8 Fig. 5: Abnormal Left kidney Uptake and Excretion--------------------------------------------------------------- 9 Fig. 6: Left Polycystic kidney with manual ROIs-------------------------------------------------------------------- 10 Fig. 7: Congenital Renal abnormalities------------------------------------------------------------------------------- 11 Fig. 8: ““Redrawn from McDonald and McCellan as reproduced by Abeshouse Bhisitkul, 1959”” (Belman et al., 202)----------------------------------------------------------------------- 13 Fig. 9: Horseshoe Kidney------------------------------------------------------------------------------------------------- 14 Fig. 10: Fused Horseshoe kidney--------------------------------------------------------------------------------------- 14 Fig. 11: “Horseshoe kidney and ureter variations” ---------------------------------------------------------------- 15 Fig. 12: Pelvic Kidney------------------------------------------------------------------------------------------------------ 16 Fig. 13: Uncrossed Renal Ectopia-------------------------------------------------------------------------------------- 16 Fig. 14: Cross-Fused Renal Ectopia------------------------------------------------------------------------------------ 17 Fig. 15: Stages of renal development--------------------------------------------------------------------------------- 18 Fig. 16: Left pelvic kidney------------------------------------------------------------------------------------------------ 19 Fig. 17: VCUG; Grade IV vesicoureteral Reflux--------------------------------------------------------------------- 20 Fig. 18 and 19: Crossed-fused renal ectopia?---------------------------------------------------------------------- 21 Fig. 20: Crossed-Fused ROI placement ------------------------------------------------------------------------------- 22
INTRODUCTION On November 22, 2008, the PAMC Nuclear medicine department performed a Tc99m-MAG₃ (Tc‑99m‑mercaptoacetyltriglycine ) Renal tubular secretion study on a female 14-20 week old patient. The patient had a recent urinary tract infection (UTI) and was being evaluated for obstructive uropathy and comorbid pathology. In addition to evaluating proximal tubular excretion, the diuretic Lasix (furosemide) was given to exacerbate any obstructive pathology. Post-acquisition processing revealed a rare anatomical abnormality called cross-fused renal ectopia. A VCUG and US revealed similar results, however a CT scan was never done to confirm the congenital anatomical anomaly. This case study will describe the nuclear medicine acquisition and processing protocol and delineate on renal anatomical anomalies.
DYNAMIC MAG-3 RENOGRAM INDICATIONS • “Congenital abnormalities in the neonate” • Evaluation of Renal perfusion and function • Diagnoses of Urinary tract obstructions • Ureterovesical/Ureteropelvic junction obstruction (UVJ/UPJ obstruction). • Renal Infection/Inflammation • Acute and chronic pyelonephritis • Evaluation of renal transplant • Hydronephrosis/Hydroureteronephrosis • Renal Vein thrombosis • Acute Renal failure • Vesicourethral reflux • Pelvicaliectasis • Hematuria • Incontinence • Abdominal pain • Palpable masses Fig. 1: Mag₃ Renogram 30 min image; [neonatal polycystic kidney]
DYNAMIC MAG-3 RENOGRAM PATIENT PREPARATION • Hydration • Hydration protocols vary from departments and institutions • [IV fluids] 5% dextrose in 0.3 normal saline; 15ml/kg over 30 minutes. Maintenance fluid volume for 200ml/kg/24hr. (Christian et al¹) • [no IV fluids] PAMC has patients begin oral hydration 30 min prior to the study. • IV and indwelling Foley catheter placement • Outpatient pediatric (neonate-14yrs old) patients undergoing renal cortical or tubular scans are required to have indwelling Foley catheter placement. Outpatient pediatric services are provided by the PAMC Pediatric Intensive Care Unit (PICU). • For infants and neonatal pediatric patients; a French 8 (2.6mmØ) or French 6 (1.8mmØ) feeding catheter may be used. • PRN Sedation per ordering physician • An outpatient appointment is scheduled with PAMC PICU to assist with pediatric sedation. • Individual institutions may use barbiturates, opiates, Phenothiazines, Neuroleptic agents, or combinations. See: Society of Nuclear Medicine Procedure Guideline for Pediatric Sedation in Nuclear Medicine. Fig. 2: 20 ml emulsion ampoule of Propofol
DYNAMIC MAG-3 RENOGRAM RADIOPHARMACUETICAL • Tc99m-MAG ₃ • Tc‑99m‑mercaptoacetyltriglycie • ERPF (Effective Renal Plasma Flow) and Proximal Tubular excretion • 90% protein bound • 40% first pass extraction • Compartmental localization • Radionuclide • Technetium-99 metastable • T½= 6.02hrs • 89% 140 keV gamma photon • R/P Dosimetry • 22mcCi/lb or 10mCi for normal adult • Target organ: Kidneys (.014 rads/mCi) • Critical organ: Bladder wall and Ovaries (.48 and .026 rads/mCi respectively) • Lowest dose /m², ideal for pediatrics <2yrs Proximal convoluted tubule Glomerulus Afferent Arteriole Efferent Arteriole Fig. 3: Renal Nephron cut-away
DYNAMIC MAG-3 RENOGRAM ACQUISITION PROTOCOL • POSITION • Image posterior. (NOTE: only image anterior if patient has renal transplant) • (1)“Center the detector’s FOV on the elbows” or (2)“Place Xiphoid and pubic symphysis in FOV” or (3)“Center on the crux of the iliac crests.” • Pediatric patients may need Papoose boards to limit motion. • Place Foley catheter out of the FOV. (NOTE: some institutions inject 20-100mcCi to improve positioning. Pediatrics don’t require this. • FLOW • 128x128 or 64x64 matrix • 2 seconds per frame for 1 minute. • DYNAMIC • 128x128 matrix • 60 seconds per frame for • Tc99m-MAG ₃ INJECTION • Oldendorf method or modified tubing extensions are used during bolus phase. • Extra tubing increases the chance of residual activity in the IV. Flush 10cc saline. • Lasix (furosemide) INJECTION • Dose: 0.5mg/kg lasix • Lasix is slowly infused over 1 minute at 10 minutes post injection of Tc99m-MAG ₃. Fig. 4: Detector FOV
DYNAMIC MAG-3 RENOGRAM PROCESSING • GE Xeleris Dynamic Motion Correction Renal Analysis Mag₃ renal with lasix Ht. and Wt. Pediatric state Initial and residual activity • Flow images are manually compressed to 8 seconds/frame. • Dynamic Images are compressed to 2 minutes/frame. Fig. 5: Abnormal Left kidney Uptake and Excretion
DYNAMIC MAG-3 RENOGRAM POST-PROCESSING PROTOCOL • ROI placement, patient motion, dehydration, and kidney location are major factors contributing to the quality of the study. • Depending on the indication, unsatisfactory time-activity curves can be produced from partially drawn kidney ROIs or fully draw kidney ROIs (Christian et al). • Some radiologists prefer exclusion of the renal pelvis when looking at renal function vs. obstruction. • Images from 4 minutes are used to calculate relative renal function. • Collecting system is included in kidney ROI • Quantitative Dynamic renal images from 2-29 minutes are used for renal time-activity curves. • Collecting system is excluded from kidney ROI Fig. 6: Left Polycystic kidney with manual ROIs
CONGENITAL RENAL ABNORMALITIES • FUSED KIDNEY • Horseshoe kidney • ECTOPIC KIDNEY • Renal ectopia without fusion • Crossed Renal Ectopia without fusion • Uncrossed Renal Ectopia without fusion • ECTOPIC FUSED KIDNEY/s • Renal Ectopia with fusion • Crossed fused renal Ectopia • Uncrossed fused renal Ectopia NOTE: Thoracic kidneys are ectopic but are associated with diaphragmatic hernias and won’t be discussed because their etiology is much different from congenital ectopic kidneys. Fig. 7: Congenital Renal abnormalities
CONGENITAL RENAL ABNORMALITIES FUSION CLASSIFICATION SCHEMES • Wilmer (1974): • 1) Horseshoe kidney • 2) L-shaped kidney that is a transitional form between horseshoe kidney and unilateral fused kidney. (the ureter does not cross the midline). • 3) Unilateral fused ectopic kidney where the ureter crosses • 4) Miscellaneous • McDonald and McClellan (1957) • 1) crossed renal with fusion • 2) crossed renal ectopia without fusion • 3) Solitary crossed renal ectopia • 4) Bilaterally crossed renal ectopia
RENAL FUSION CLASSIFICATION McDonald and McClellan (1957) Fig. 8: ““Redrawn from McDonald and McCellan as reproduced by Abeshouse Bhisitkul, 1959””
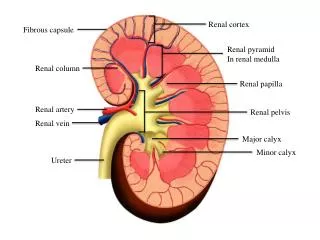
HORSESHOE KIDNEY ANATOMY • Horseshoe kidney is the most common congenital renal ectopia. (1 in 450 people). • 90% are fused in the lower moieties. • Kidney stones and Ureteropelvic junction (UPJ) obstruction are common in Horseshoe kidney . • This kidney is the only ectopic anomaly that remains in the ipsilateral retroperitoneal space. Fig. 10: Fused Horseshoe kidney Fig. 9: Horseshoe Kidney
HORSESHOE KIDNEY VARIATIONS Fig. 11: “Horseshoe kidney and ureter variations”
ECTOPIC PELVIC KIDNEY • Pelvic kidneys’ have a similar occurrence rate as horseshoe kidney (1 in 500). • Frequent problems associated with pelvic kidneys are UTIs and vesicourethral reflux. • Unlike Horseshoe kidney, ectopic pelvic kidneys “lay” outside the ipsilateral retroperitoneal space and renal fossa. • Pelvic kidney’s are classified as Uncrossed/Solitary Ectopic kidneys without fusion. Fig. 13: Uncrossed Renal Ectopia Fig. 12: Pelvic Kidney
CROSSED-FUSED RENAL ECTOPIA • Depending on the source, crossed-fused renal ectopia has an incidence of 1 in 14,000 pediatric admissions and 1 in 7,500 autopsies. • Incidence of VUR (Vesicoureteral reflux) is estimated at 70% • Hydronephrosis is reported at 33-50%. Fig. 14: Cross-Fused Renal Ectopia
Renal Ectopia Embryological Etiology • The exact cause of renal ectopia is still unknown. • “Normal morphogenesis requires the coexistence of competent inducible constituents which are under strict temporal control. • Teratogenic agents like thalidomide increase the risk of developing ectopic kidneys. • Congenital abnormalities like: spinal deformities and anorectal anomalies are associated with renal ectopia. • Studies and research show inhibition of embryological development in the early stages decreases renal blastema growth and retards the growth of ureteric buds. • Time-lag theory: A genetic error causes the metanephric blastema to develop out of sync with the ureteric bud. Fig. 15: Stages of renal development
PATIENT HISTORY • The female 14 week old pediatric patient with crossed-fused renal ectopia had a history of UTI. • An abdominal Ultrasound (US), voiding cystourethrogram (VCUG), and MAG₃ renogram w/ lasix were ordered consecutively. • The US showed an small ectopic pelvic kidney. A VCUG showed reflux into the left ureter. Fig. 16: Left pelvic kidney
IMAGE FINDINGS • Ultrasound: • Pelvic kidney • Voiding Cystourethrogram (VCUG): • Grade II vesicoureteral Reflux • MAG₃ renogram • Ectopic pelvic kidney with decreased size and function. Fig. 17: VCUG; Grade IV vesicoureteral Reflux
IMAGE FINDINGS: MAG₃ Renogram 5 MIN • MAG₃ and lasix dose: • 1mCi Tc99m-MAG3 (22mcCi/lb) • Minimum 1mCi • 6mg lasix @10 minutes • Crossed-fused Renal ectopia was never diagnosed because a corresponding CT was not performed • However, the possibility of crossed-fused ectopia was very high. • MAG₃ renography showed no obstruction but decreased “left”/ “pelvic” kidney function. • Obvious ectopic kidney with possible fusion. 25 MIN Ectopic kidney Bladder Fig. 18 and 19: Crossed-fused renal ectopia?
IMAGE FINDINGS: MAG₃ Renogram 5 MIN • Processing the images were difficult and required accurate placement of the ROIs. • The anatomical anomaly caused the left and right kidney ROIs to overlap. • In addition to overlapping structures; the RT renal pelvis was very difficult to mask from renal parenchyma. • The time-activity curve revealed slight variations from patient motion and the above mentioned artifacts. 25 MIN Fig. 20: Crossed-Fused ROI placement
CONCLUSION Crossed fused renal ectopia is a very rare congenital abnormality. Positioning, ROI placement, and other imaging considerations should be discussed with the radiologist or ordering physician. The case presented was not confirmed as “crossed fused renal ectopia” because CT imaging was not done. After consulting with the Radiologist, he recommended a Tc99m-DMSA renal SPECT to assess renal cortical function.
REFERENCES Belman, A. Barry, Lowell R. King, Steven A. Kramer (2001). Clinical Pediatric Urology. London, England: Martin Dunitz Ltd. Christian, C., & Donald, B. (2004). Nuclear Medicine and PET Technology and Techniques.St. Louis, Missouri: Mosby. Jain, P., & Parelkar, S. (2008). Uncrossed complete ureteral duplication with dysplastic lower moiety: A violation of the Weiger--Meyer law. Jounal of Pediatric Urology. 4, 404-406. Guarino, N., & Tadini, B. (2004). The Incidence of Associated Urological Abnormalitites in Chilren with Renal Ectopia. The Journal of Urology. 172, 1757-1759. Rinat, C., & Farkas, A. (2001). Familial inheritance of crossed fused renal ectopia. Pediatric Nephrology. 16, 269-270. Ghosh, B., & DeSantis, M. (2008). Crossed Fused Renal Ectopia with Calculi. American College of Surgeons. 10, 753. Gu, L., & Alton, D. (1991). Crossed Solitary Renal Ectopia. Urology. XXXVIII, 556-558. Felsenberg, J., & Nasrallah, P. (1991). Crossed Renal Ectopia Without Fusion Associated with Hydronephosis in an Infant. Urology. XXXVIII 5, 450-452. Arena, F., & Arena, S. (2007). Is a complete urological evaluation neccessary in all newborns with asymptomatic renal ectopia?. International Journal of Urology. 14, 491-495. Hendren, W. H., & Donahoe, P. (1976). Crossed Renal Ectopia in Children. Urology. VII #2, 135-139. Mohseni, M. G., & Aghamir, S.K. (2002). A rare case of renal ectopia: a thoracic kidney with stone formation. British Journal of Urology International. 90, 1.
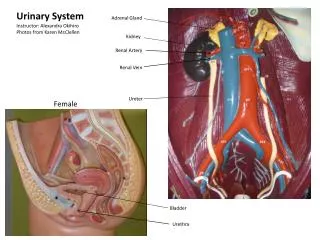
REFERENCES Ell, P. J., & Gambhir, S. S. (Eds.). (2004). Nuclear Medicine in Clinical Diagnosis and Treatment Volume 2. London, England: Churchill Livingstone. Netter, Frank H. (2006). Atlas of Human Anatomy, 4th Edition. Philadelphia, PA: Saunders. Nucleus Medical Art (2009). Female Abdomen with Kidneys, Renal Vessels, and Uterus: Cut-Away View. SMART Imagebase. Retrieved May 10, 2009, from http://ebsco.smartimagebase.com/generateexhibit.php?ID=2271 Nucleus Medical Art (2009). Anatomy of Renal Tubule and Vasculature. SMART Imagebase. Retrieved May 10, 2009, from http://ebsco.smartimagebase.com/generateexhibit.php?ID=23398 Children's Memorial Hospital, Institute for Fetal Health (August 2008). Fetal Pelvic Kidney and Horseshoe Kidney. Retrieved May 4, 2009, from Children's Memorial Hospital Web site: http://www.childrensmemorial.org/depts/fetalhealth/pelvic_kidney.aspx Chilren's Memorial Hospital; Chicago, IL, (August 2008). Fetal pelvic kidney and horseshoe kidney. Retrieved May 5, 2009, from Institute for Fetal Health Web site: http://www.childrensmemorial.org/depts/fetalhealth/pelvic_kidney.aspx Fairman, (2003). Pediatric Condition: Abnormalities. Retrieved May 10, 2009, from www.urologyhealth.org Web site: http://www.urologyhealth.org/pediatric/index.cfm?cat=01&topic=121&drawings=yes Hill, Dr. Mark (2007). UNSW Embryology Beginnings, Growth and Development Practical Sexual Differentiation - 5. Retrieved May 10, 2009, from The University of New South Wales; Sydney, Australia Web site: http://embryology.med.unsw.edu.au/Medicine/BGDlabXYXX_5.htm NIDDK Image Library, (uknown). Ectopic Kidney (KU-234). Retrieved May 10, 2009, from www.niddk.gov Web site: http://www.catalog.niddk.nih.gov/imagelibrary/detail.cfm?id=595
REFERENCES Mandell, G. A., & Majd, M. (2003). Society of Nuclear Medicine Procedure Guideline for. SOCIETY OF NUCLEAR MEDICINE PROCEDURE GUIDELINES MANUAL. 3, 174-177. Yoshida, J., & Tsuchiya, M. (2003). Mass screening for early detection of congenital kidney and urinary tract abnormalities in infancy. Pediatrics International. 45, 142–149. Shulkin, B. L., & Mandell, G. A. (2008). Procedure Guideline for Diuretic Renography. Journal of Nuclear Medicine Technology. 36, 162-168. Milford, M. (2007). Renal Abnormalities. Retrieved May 6, 2009, from www.tofs.org.uk Web site: http://www.tofs.org.uk/index.php/what_is_tof_oa/about_vacterl/vacterl_-_renal_anomalies Watanabe, Toru (2002).Reflux nephropathy in a patient with crossed renal ectopia with fusion. Pediatric Nephrology. 17, 617-619. Rakoczi, E., & Sandor, T. (2009). Association of Renal Ectopia With Fabry's Disease in 3 Patients. The Journal of Urology. 181, 1949-1954. Garne, E., & Loane, M. (2009). Congenital hydrocephalus - prevalance, prenatal diagnosis and outcome of pregnancy in four European regions. European Journal of Paediatric neurology. XXX, 1-6. Friedland, G. W., & De Vries, P. (1975). Renal Ectopia and Fusion. Urology. V, 698-706. Pak, K., & Konishi, T. (1988). Noncrossed Renal Ectopia with Fusion associated with Single Ectopic Ureterocole. Urology. XXXII, Number 3, 246-249. MediaWiki.org, (2008). Crossed-fused renal ectopia. Retrieved May 10, 2009, from www.radwiki.net Web site: http://www.radswiki.net/main/index.php?title=Crossed-fused_renal_ectopia#Discussion_of_Crossed-fused_renal_ectopia NIDDK Image Library, (uknown). Ectopic Kidney (KU-234). Retrieved May 10, 2009, from www.niddk.gov Web site: http://www.catalog.niddk.nih.gov/imagelibrary/detail.cfm?id=594