Download
1 / 1
10 likes | 137 Views
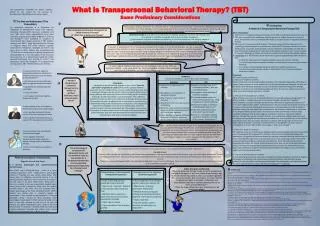
What is Transpersonal Behavioral Therapy? (TBT) Some Preliminary Considerations. This presentation illustrates an article, recently written by the author for the Journal of Transpersonal Psychology on the same subject. The Aims and Addressees of This Presentation:. . Conclusions:

E N D
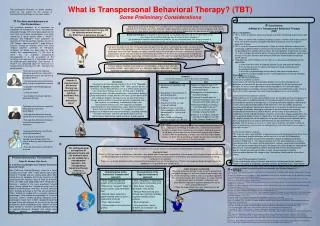
What is Transpersonal Behavioral Therapy? (TBT) Some Preliminary Considerations This presentation illustrates an article, recently written by the author for the Journal of Transpersonal Psychology on the same subject. The Aims and Addressees of This Presentation: Conclusions: A Model of a Transpersonal Behavioral Therapy (TBT) Taking about „behavioral therapy“ we nowadays refer to “cognitive-behavioral therapy” and not to the methodically reductionism of the 60ths and 70ths. Although modern behaviorists tend to be more and more integrative and eclectic, there are still some typical characteristics constitutive of behavioral approaches. An appropriate definition could be: [2] No systematic proposals of a framework for integration of transpersonal issues into cognitive-behavioral therapy (CBT) have been published until now. After some basic considerations have been uttered by a group around Miller & Martin[15], D’Souza and Rodrigo[16] have published on questions of meaning and their religious answers in CBT. Nielsen, Johnson and Ellis[17] apply Rational-Emotive Therapy on religious clients and utilize religious cognitive schemata for therapeutic strategies (as before has been done by other authors less comprehensively [18]). But none of these has an explicitly transpersonal presupposition (i. e. the assumption of the existence and relevance of a transcendent reality for whole-personal well-being). Only recently, H. Piron[19] has speculated about the necessity of a transpersonal turning point in CBT. Therefore this poster intends … Can transpersonal behavioral therapy still be called behavioral therapy? Or: What then is behavioral therapy? • Basic assumptions: • TBT is a form of cognitive-behavioral therapy and fulfills all defining requirements to be one. • TBT does not conflict with traditional religious systems. It neither claims to be a part of them, nor do their contents contradict theoretical or practical issues of cognitive behavioral therapy. • TBT is a part of transpersonal therapies, if these are not by definition reduced to the psychology of altered states of consciousness, because TBT’s primary intention is not the development of superior spiritual states, but the integration of spirituality into daily life. It thus includes the spiritual work in all levels of therapeutic endeavor, even in basic therapy of “secular” disorders and does not divide into mental health and spiritual growth phases. • Indications for a TBT therefore are the same as in general psychotherapy with the adjunct that • a) either the client wants to integrate spiritual issues and common therapy, • b) or she/he perceives his spiritual development being stuck because of psychological problems, • c) or his/her symptomatology derives directly from spiritual experiences, • d) or her/his symptomatology results in unfavorable forms of (pseudo-)religious behaviors or beliefs. Behavioral therapy is a (a) planed, (b) structured, (c) explicitly purposeful (d) set of interventions, that (e) is based on scientific knowledge and (f) aimed at direct changes of (g) dysfunctional cognitive and behavioral patterns, (h) into functional ones, this doing by means of (i) cognitive and behavioral restructuring, (k) self-control, and (i) real and imagined exercise. If we want to establish any form of transpersonal therapy that is based on a behavioral paradigm, we have to keep the elements of this definition in mind. One part of it has to be outlined further: What does “based on scientific knowledge” mean? As Tart[3] already has stated, scientific study of altered states of consciousness or of “unusual experiences” can be one such a task of a scientifically grounded TBT. But there are contributions of neighboring disciplines, too. For example, psychology of religion provides us with empirically examined theories like “learning of spirituality” by imitating models [4], represented in schema networks [5]. In dead, religious traditions have used learning techniques as part of their spiritual instruction method – some more, some less. Moreover, cognitive behavioral therapists have been inspired by Buddhism and thus have an implicit relationship to it. • To demonstrate to the cognitive-behavioral practitioner, interested in transpersonal issues, but not daring to practice them[1]… • …that transpersonal psychotherapy within a cognitive-behavioral setting • is possible and methodologically „permitted“ • is easy to realize • can be good structured cognitive-behavioral therapy Procedure: TBT uses four sets of elements: 1) The set of “profane” contents Clients come with common psychological problems of our days like depression, difficulties to relate to other persons or sexual dysfunction. As for the transpersonal therapist, his duty is to be able to deal with these problems on a level of modern psychopathological knowledge, personal competence and modificational skills (set 3+4). But also the clients personal and social resources belong to this set of contents. 2) The set of “transcendental” contents Other problems are of a more transcendental level, for example spiritual emergencies[12] or feeling unable to meditate because of ruminative thoughts. Among the (“negative”) transcendental contents of therapy may as well be dysfunctional cognitions deriving out of one’s own religious belief system. At the same time, this set contains all spiritual resources of the person. We are here dealing with inner-psychic or attitudinal elements, like thoughts or attitudes referring to a concept of the transcendent; the emotional relationship to the divine or a spiritual teacher; certain states of consciousness like mindfulness (smriti) or deep meditation (dhyana); and all other religious propositions that form a personal religious schema. Though they may be important features of a spiritual life, religious actions are not the object nor the psychic prerequisite for spirituality but a form of practicing it or it’s method, and therefore are discussed below as spiritual methods.With this division we more or less follow a basic distinction, formulated in occidental terms as one between vita activa and vita contemplativa or in the Hindu tradition karma yoga vs. other forms of yoga[13]. 3) The set of “profane” methods TBT uses the same set of methods as cognitive behavioral therapy generally does. It just adds some more specific techniques which are fully in line with the fundamental behavioristic assumption of cognitive and actional change by applying systematic learning methods (set 4). This means that they start their work making an anamnesis containing a map of the clients actual and previous religious experiences and attitudes. Than transpersonal behavioral therapists will analyze the clients problems (knowing that they are just evolving hypotheses) before planning what they do (knowing that the present moment can interrupt all plans as well), always keeping in mind the interconnections between the religious map, the problem sketch and the intervention sketch. 4) The set of “transcendental” methods To this set belong all actional elements and spiritual methods provided by traditional religions like prayer or meditating, attending services, performing rituals, and ethically valuable actions. On the other hand, spiritual psychotherapies have developed some original methods for enhancing spiritual processes, like Roberto Assagioli’s[14] techniques. Buddhism… …has diverse relations to cognitive-behavioral methodology: I wonder if transpersonal behavioral therapy has any relation to spiritual traditions. Has it any precursors there? Christianity… …developed a spiritual training program in form of the “Exercitia Spiritualia” by Ignatius of Loyola (1491-1556). Ignatius delivers a systematic manual, being the basis of a four weeks training course. Like in behavioral therapy manuals, the first step is to identify dysfunctional habits, attitudes and behaviors, the second is building up the motivation of change. And like sometimes a new identification with a different cognitive concept may be the aim of behavioral therapy, Ignatius guides his exercitant by active imagination into a new vision as a saved being, fundamentally living in the consciousness of God’s love. This happens by repeated contemplation of a new-testamentary scene, which the exercitant paints more and more plastically. This program is an ancient predecessor of modern covert control techniques, including methods like covert extinction, and even self-observational and self-reinforcement methods like a daily record are already applied. • To demonstrate to the non-cognitive-behavioral transpersonal psychologist: • that cognitive-behavioral therapy can be of use for transpersonal aims • that cognitive-behavioral therapy is a part of the transpersonal movement But if you don’t mind I would like to add, that transpersonal therapists are not a subdiscipline of theology or Buddhismus. Confessional neutrality is our duty in respect to our multiconfessional clients. And being a part of psychology, we are more closely affiliated with comparative religious studies or with the psychology of religion than with any single religion, whereas we differ from psychology of religion by our clear statement for the existence of the transcendent. • To demonstrate to the scientifically oriented psychologist: • that cognitive-behavioral transpersonal therapy meets the criteria of being a part of behavioral therapy • that a lot of research is possible in this area The anthropological conceptions of behavioral theory and the method it uses are not suitable for a transpersonal approach. Can transpersonal behavioral therapy really be a transpersonal therapy? • I don’t agree that we differ in respect to our concept of man or real practice of client-therapist relationship. • Concept of man: • Clients in CBT are seen as autonomous, that means: they decide about major goals and contents of the therapy, they do something for themselves, not the therapist does it for them. They are self-responsible and therefore active partners of therapists (this contrasts to behaviorists as being manipulative rats-doctors) • There is a continuum between healthy and unhealthy or disturbed forms of mental processes. There is no categorical border between normal or abnormal as it is psychiatry or psychoanalysis. Personal Introduction: The presenter… Edgar W. Harnack, Dipl.-Psych. is a German psychologist and cognitive-behavioral psychotherapist. Born 1968 near Freiburg/Germany, I went to a Jesuit boarding school from 1979 – 1988, where I took a great interest in Theology and was socially quite active. After having done my obligatory community service in an old styled psychiatric hospital, I went to Chile for 8 months in the vain hope to do good deads there. Being back in Germany I worked in the same psychiatric hospital again, having noticed that I wanted to resign from the medical university place I had then. And one semester later I studied psychology at the Freie Universität Berlin. 1996 I finished my studies with a university degree as psychologist. I then worked as psychologist in a forensic psychiatry, where I ended up being temporary chief-psychologist 4 years later. In 2001 I decided it would not be good to live with criminals for the rest of my life and changed to a quiet rehabilitation clinic, where I still work today. Beside it I finished a certified additional training as cognitive-behavioral therapist and attend some private patients psychotherapeutically in Berlin/Germany. Client-therapist relationship: Cognitive-behavioral therapy’s main accent in professional training of therapists as well as in theory of course does not lie on the relationship, which is seen as a customer-provider like same-level-relation. But nevertheless, it is clear, that the 3 Rogerian principles of empathy, authenticity and unconditioned regard are important prerequisites for all forms of psychotherapy[11]. If there are major differences, they, tentatively, can be outlined as follows: References: [1] Hutton, M. S. (1994). How transpersonal therapists differ from other practitioners: An empirical study. Journal of Transpersonal Psychology, 26 (2), 139-174 [2] www.nacbt.org/whatiscbt.htm and: Margraf, J. (1997). Möglichkeiten und Grenzen der Verhaltenstherapie. In: K. D. Hildemann & P. Potthoff (ed.): Psychotherapie – Quo vadis? Göttingen: Hogrefe [3] Tart, C. T. (1975). Science, states of consciousness, and spiritual experiences: The need for state-specific sciences. In: C. T. Tart (ed.): Transpersonal psychologies. New York: Harper & Row [4] Oman, D. & Thoresen, C. E. (2003). Spiritual modeling: A key to spiritual and religious growth? The International Journal for the Psychology of Religion, 13 (3), 149-165 [5] McIntosh, D. (1995). Religion-as-schema, with implications for the relation between religion and coping. The International Journal for the Psychology of Religion, 5 (1), 1-16 [6] Berzin, Alexander (1998). Developing Balanced Sensitivity: Practical Buddhist Exercises for Daily Life. Ithaca, Snow Lion.Nissanka, H. S. (1993). Buddhist Psychotherapy. New Delhi: Vikas Publishing House [7] Kanfer, F. H., Reinecker & D. Schmelzer (2000). Selbstmanagement-Therapie: Ein Lehrbuch für die klinische Praxis, 3. Aufl. Berlin: Springer [8], [9] McIntosh, W. D. (1997). East meets west: Parallels between Zen Buddhism and social psychology. The International Journal for the Psychology of Religion, 7 (1), 37-52 [10] Ellis, A. (1975, 9th ed.). Reason and Emotion in Psychotherapy. Secaucus, N. J.: Lyle StuartLinehan, M. (1993). Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York: Guilford PressZindel, S. V., Williams, J. M. , Teasdale, J. D. (2002). Mindfulness-Based Cognitive Therapy for Depression : A New Approach to Preventing Relapse. New York: Guilford Pub [11] Zimmer, D. (2004). Wie arbeiten Verhaltenstherapeuten mit der therapeutischen Beziehung. Psychotherapie im Dialog, 5 (4), 335-340 [12] Grof, S. & Ch. Grof (ed.) (1989). Spiritual Emergency: When personal transformation becomes a crisis. New York: Tarcher [13] Vivekananda, Swami (1982). Karma-Yoga and Bhakti-Yoga. New York: Ramakrishna-Vivekananda Center [14] Assagioli, R. (1965). Psychosynthesis – a manual of principles and techniques. New York: Hobbs, Dorman & Co [15] Miller, W. R. & Martin, J. E. (1988): Behavior therapy and religion. Integrating spiritual and behavioral approaches to change. Newbury Park: Sage [16] D’Souza, R. F. & Rodrigo, A. (2004). Spiritually augmented cognitive behavioral therapy. Australasian Psychiatry, 12 (2), 148-152 [17] Nielsen, S. L., Johnson, W. B. & Ellis, A. (2001). Counseling and psychotherapy with religious persons. Mahwah: Lawrence Erlbaum [18] Johnson, W. B. (1992). Rational-emotive therapy and religiousness: A review. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 10 (1) [19] Piron, H. (2005). Meditatives Gewahrsein in der Verhaltenstherapie: Auf dem Weg zu einer Transpersonalen Wende? In W. Belschner, H. Piron, H. Walach (Ed.), Bewusstseinstransformation als individuelles und gesellschaftliches Ziel. München: LIT