Download
1 / 64
640 likes | 827 Views
Dive into the world of endocrine diseases with Prof. M.K. Hamam in Burket’s Tenth Edition, covering hormonal disorders like Addison’s disease, thyroid disorders, diabetes mellitus, and more. Explore the intricate hierarchy of the endocrine system and the role of the hypothalamus, pituitary gland, and adrenal gland in maintaining hormonal balance. Learn about pituitary gland disorders, oral manifestations, and implications for dental evaluation and management. Gain insights into adrenal gland disorders, such as Addison's disease and Cushing's syndrome, along with their clinical features and management. Discover how these disorders impact dental treatment and patient care.

E N D
ENDOCRINE DISEASE Prof. M.K.Hamam Oral Medicine Diagnosis & Treatment Burket’s Tenth Edition
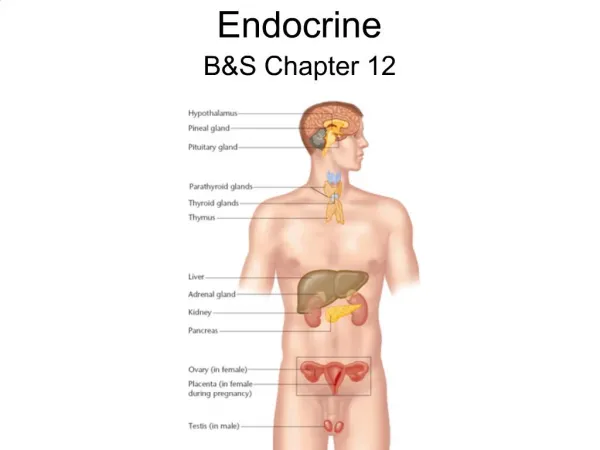
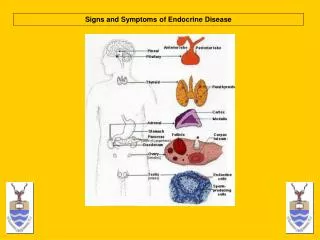
1- Endocrine Disorders • Importance of hormones • Endocrine system • Hormonal disorders • Adrenal gland disorders • Addison’s disease • Dental evaluation, management • Thyroid disorders • anatomy - Location • Hormone • Hypothyroidism • Hyperthyroidism • Dental evaluation and management • Diabetes mellitus • 2- liver diseases
Introduction Endocrine system are inherently hierarchically organized . The hypothalamus controls the pituitary gland activities which in turn regulate other endocrine gland secretions . Hypothalamus secretes releasing and inhibiting factors . Among the releasing hormone is corticotrophin releasing factor ( CRF ) , which stimulates the release of adrenocorticotrophic hormone ( ACTH ) from the pituitary gland .
Hierarchical arrangement ACTH acts on adrenal cortex to cause the release of cortisol ( hydrocortisone ) Hypothalamus secretes → CRF stimulates → pituitary gland secretes→ ACTH stimulates → Adrenalcortex → Secretes → Cortisol .
Negative feed back regulatory All endocrine system functions as a closed loop . In most endocrine system ,negative feed back regulatory their function . For example , hypothalamus and pituitary gland stimulate the secretion of cortisol from adrenal cortex . While cortisone inhibits hypothalamus and pituitary gland secretion ( negative feed back ).
Pituitary gland • The anterior lobe of pituitary gland produces . • 1- AdrenoCorticotrophic Hormone ( ACTH ) • 2- Melanocyte Stimulating Hormone ( MSH ) • 3- Thyroid Stimulating hormone .( TSH ) • 4- Growth Hormone ( GH ) • 5- Follicle Stimulating Hormone ( FSH ) • 6- Luteinizing Hormone ( LH ) • 7- Prolactin
A- Disorders of pituitary gland ( Dwarfism ) • General manifestation • 1- Impaired growth of child ( GH ) • 2- Hypoadrenocorticism ( ACTH ) • 3- Hypothyroidism ( TSH ) • 4- Failure of ovulation , amenorrhea . ( FSH ) • 5- Impotence , defective spermatogenesis .( LH ) • 6- Failure of lactation ( - prolactin )
Oral manifestation :- • 1- Delayed shedding & eruption of teeth . • 2- Microdontia : if occurs before odontogensis . • 3- Crowding and malocclusion with normal size of teeth. If occurs after odontogenesis. • Dental implication :- • Stress, surgery , GA,infection ,sedative ,hypnotic , and trauma • May precipitate hypo pituitary coma . • Hypo pituitary is related to decrease TSH & ACTH , so the patient cannot tolerate stress. • Hypo pituitary coma is manged by :- • 1- 200 mg hydrocortisone sodium succinate I.V. • 2- 25-50 mg dextrose ( if there is hypoglycemia ) • 3- Oxygen • 4- Call ambulance for hospital admission .
B- Hyperpituitarism • Children ( before epiphysis closure ) → Gigantism • 1- well proportional individual but huge . • 2- teeth spacing ( if occur after odontogensis ) • Adult :- ( after epiphyseal closure ) → Acromegaly • 1- large hand , feet , malar bone , supraorbital ridges , tongue , lip, mandible prognathism ) • 2- Teeth : spacing ( food impaction ) • hyper cementosis ( teeth fracture , or difficulty in extraction )
A 12 year old boy, 6’5”, with his mother, and his hand (left) in comparison with that of a grown man, 6’1” All long bones in the body effected before closure of epiphyseal growth plates
Dental implication • 1- systemic problem associated with hyperpituitrism may complicate the dental treatment as :- • Hypertension • Diabetes mellitus • Hypercalcemia • Cardiomyopathy . • 2- Hazards of GA related to breathing problem where :- • Tongue is large • Epiglottic opening is narrow . • Kyphosis . • Thymus gland is enlarged • So it is better to avoid supine position .
Adrenal gland • Adrenal gland secrete :- A - From medulla 1- Epinephrine ( adrenaline ) 2- nor epinephrine ( noradrenalin ) B- From Cortex 1- Glucocorticoids ( cortisol ) 2- Mineralocorticoids ( aldosterone ) 3- Sex hormones .
Disorders of adrenal gland • 1- Adrenal cortex insufficiency • Etiology • 1- Congenital • 2- Acquired • A- Primary : Addison’s disease • B- Secondary :- ● to exogenous steroid therapy . • ● to pituitary insufficiency . ( ACTH deficiency )
11-Adrenal cortex hyperfunction : • Etiology • A- Cushing disease • It is due to pituitary gland adenoma resulting in increase ACTH • That stimulate adrenal cortex . • B- Cushing syndrome : • It is due primary adrenal adenoma . • C- Iatrogenic Cushing syndrome • It is due to exogenous corticosteroid therapy .
Clinical Features of Cushing’s Syndrome Round (“moon”) face. A hump on upper back Buffalo hump stretch marks on their abdomen (“striae”) Hypertension Prolonged wound repair Obesity Mental depression
Easy bruising Thinning skin Poor wound healing Acne Purple striae Hirsutism Female balding Menstrual irregularity Sleep disorders Excessive hunger Excessive thirst Frequent urination Sweating Anxiety Confusion Concentration loss Memory loss Depression Suicidal thoughts Panic attacks Abdominal weight gain Red, round ‘moon’ face Thinning extremities ‘Buffalo hump’ High blood pressure High blood sugar Muscle weakness Osteoporosis/Fractures Infections Blood clots Visual field defects
A – Primary Adrenal cortex insufficiencyAddison’s disease • Definition • It is adrenal cortex insufficiency ( atrophy ) leading to failure of cortisol and aldosterone secretion . • Auto immune disease : due to circulating antibodies directed against adrenal cortex . • Tuberculosis • Sarcoidosis • Hemorrhage • Histoplasmosis • Malignancy . Amyloidosis
Clinical Features • Manifestations related to low level of aldosterone • 1- Sodium & water depletion • 2- Reduced extracellular volume & hypotension . • 3- Retained potassium & hydrogen ions • 4- Hyperkalemia & acidosis . • Manifestaion related to low level of cortisol • 1- Stimulation pituitary gland to secrete pro-opio melanocortin . So there is increased level of :- • Melanocyte stimulation activity which lead to increase skin & oral melanin pigmentation . • ACTH .
Peutz–Jeghers syndrome: multiple pigmented spots on :- Addison disease: pigmentation of the :-. the skin. the lower lip. buccal mucosa gingiva the buccal mucosa. lower lip
2- Hypoglycemia • 3- Weight loss , weakness • 4- Addisonian’s Crisis ( adrenal crisis ) • It is manifestationby sever exacerbation of symptoms as hypotension , headache , dehydration , weakness , nausea , vomiting . • It is precipitated by factors that increase the body demand for cortisol such :- as surgery , stress , infection , trauma , G.A . • The patient may die if not treated immediately . • Laboratory finding • Cortisol , Sodium • ACTH , Potassium .
B- Secondary adrenal cortex insufficiency ( patient on glucocorticoid therapy ) • Pharmacological action of glucocorticoids • 1-Owing to their anti- inflammatory and immune- suppressive action , • There are prescribed for management of :- • Allergic diseases . • Autoimmune diseases : ( Lupus erythematosus , pemphigus vulgaris ,…..) • 2- they are prescribed as replacement therapy in patients with Addison ‘s disease
Complications of glucocorticoid therapy • A- Adreanal cortex atrophy :- • The long term low dose steroid ( 10 mg prednisone for one month ) or short term high dose steroid results in adrenal cortex suppression ( atrophy ). • Adrenal cortex secretion is under the control of ACTH secreted by pituitary gland . • Exogenous steroid received by the patient for management of certain allergic or skin disease results in suppression of ACTH release . In turn , endogenous adrenal cortex secretion is suppressed and the adrenal glands under atrophy . • .
Patients with adrenal cortex atrophy cannot tolerate stress , surgery , G.A , infection , and trauma . There is increase in the body with such high levels of endogenous corticosteroids ( 300 mg ) , so the patient suffers adrenal crisis . • Causes of adrenal crisis :- • 1-Adrenal insufficiency (A- cong. Adrenal ins .B- Primary : Addison's disease .& C-Secondary: ,exogenous steroid , surgical excision of gland , pituitary insufficiency ) + certain condition ( stress, G.A ., infection , surgery , trauma ) → adrenal crisis . 2- Sudden withdrawal of exogenous steroid
How to avoid adrenal atrophy ? • 1- alternate day : on the day off therapy , the adrenal pituitary axis is allowed to function and produce endogenous cortisol . • 2- single morning dose of exogenous steroid 1.5 hrs. after arising . Cortisol level is normally high in the morning . Thus if steroid is given at this time it does not to tend to suppress ACTH and adrenal gland secretion . • How to avoid adrenal crisis ? • 1- Careful case history :- • It should be remember that not only patient under current treatment are not at risk of adrenal crisis but also patient who had steroid therapy during the last year ( normal function of adrenal gland is restored within 9-12 month. ) • 2- Supplementary corticosteroid should be given before and during period of stress ( G.A. Trauma ,…… ) • 3- Gradual withdrawal of steroid therapy to allow for the restoration of adrenal function.
Management of patient on steroid therapy . • Under local anaesthesia • 1- patient on total replacement therapy : ‘’ Addison’s disease ‘’ • Hospitalization • It is better to over treat ( i.e. high dose of steroid ) during surgery rather that to have Adrenal crisis . • 2- patient received steroid during the previous 12 months . • 200 mg hydrocortisone orally 2 hours pre-operative or • 200 mg hydrocortisone I.V . Immediately pre operative . • 3- patient currently on steroid therapy :- • A- Short appointment : ( < 1hr. ) • Emergency → 200 mg hydrocortisone I.V . → immediately before appointment • No emergency → double the steroid dose the night and the whole day of app.
B- long appointment : ( > 1 hr. ) • Emergency → 200 mg hydrocortisone I.V. immediately before app. • 200 mg hydrocortisone I.M. 6 hrs . For 24 hrs . • No emergency → Triple the dose the night before and the whole day of app. • then gradual tapping to regular dose over the 2th of 3rd postoperative days
11- Under General Anaesthesia 1- patient on total replacement therapy : ‘’ Addison’s disease ‘’ • 2- patient received steroid during the previous 12 months . • 100 - 200 mg I.V. hydrocortisone sodium succinate with pre-medication and then every 6 hrs . For 24-72 hrs . Then continue normal medication . • 3- patient currently on steroid therapy :- • Monitor blood pressure during surgery & recovery . • I.V. steroid should be given if there is fall in blood pressure
Thyroid gland ●Thyroid glands secrete thyroxin ( T4 )and Tri- iodothyronine ( T3 ). • Thyroid gland secretion is under the control of pituitary gland which secrete ( TSH ) . The release of TSH from pituitary gland is regulated by thyrotrophine releasing factor ( TRF ) from hypothalamus . • Negative feed back mechanism similar to the pituitary adrenal axis is also regulating the thyroid gland secretion and the axis is called pituitary thyroid axis. • Hypothamus →→ secretes TRF → → Stimulates pituitary →→ secrete →→ stimulates TSH → Thyroid • Inhibit ( -ve feed back ) T3 & T4 secretes stimulate • Thyroid • The precise role of thyroid hormones is not known . However , excessive secretion increases the basal metabolic rate ( BMR )
Disorders of thyroid gland :- • Hyperthyroidism ( thyrotoxicosis ) • Types :- • Grave ‘s disease : characterized by : diffused enlargement of thyroid • gland . • : exophthalmos . • Nodular Goiter : characterized by : less sever nodular enlargement of • thyroid gland . • No exophthalmos • General manifestation • Warm moist skin • Tremors of hands and tongue • Exophthalmoses which may persist even after treatment . • Nervousness • Tachycardia . Due to increase BMR .
Oral manifestation • Normal growth of jaws • Early shedding of deciduous teeth • Early eruption of permanent teeth . • Osteoporosis . • Dental implication 1-Treatedthyrotoxic patient present no problem in dental treatment . • Untreated patient may have tachycardia and arrhythmia that can lead to heart failure . Adrenergic receptors are very sensitive to adrenaline , so local anesthesia should be free from adrenaline . Prilocaine containing octapressin is an alternative . 2- G.A ( risk of arrhythmia ) 3- anti- thyroid drugs ( thiocarbamides ) induces agranulocytosis →oral & oropharyngealulceration .
3- Thyroid crisis • It is an exaggerated manifestation of hyperthyroidism . • Precipitation factors . Stress , infection , surgery . • Clinical manifestation :- • nausea , vomiting , profuse sweating ,Tremor ,Tachycardia ,Fever , hypotension ,Finally heart failure and death. • How to avoid thyroid crisis . • Stress , ( Tranquilizers :benzodiazepine potentiate the antithyroid drugs ) • Acute infection should be managed immediately . • How to manage thyroid crisis ? • call ambulance for hospitalization since medical treatment will include :- • Hydrocortisone 200 mg i.v • Glucose i.v • Ice pack , wet pack , fans • Antithyroiddrugs and adrenergic antagonizer ( propanolol ) • N.B :-The dentist should cool the patient with cold towels and give 100-300 mg .i.v . Hydrocortizone and will be ready to initate cardiopulmonary resuscitation if indicated.
2- Hypothyroidism • Less common than hyperthyroidism • Females. • Children Cretinism(inherited or acquired) • Adult Myxedema (acquired). • Causes : • Thyroid ,Congenital absence or defect • Iatrogenic • Iodine deficiency • Chronic thyroditis • Pituitary ( secondary) • Hypothalamic (tertiary )
Cretinism • In childhood severe developmental defects (unless recognized and treated early). • Clinical manifestations • Growth retardation • Mental retardation • Mongoloid faces. • Protuberant abdomen • Delayed bony and dental development. • Defective development and maturation of the CNS • Delayed eruption of teeth. • Micrognathia • Macroglossia • Malocclusion , anterior open bite • Puffy , enlarged , protruded lip. • Short & flat nose
Myxedema • Myxedema is defined as hypothyroidism acquired (not inherited) in the adult. • Decreased metabolism “hypothyroid state”. • Facial edema(myxedema). • Coarse skin. • Decreased mental acuity. • Physical activity, and tolerance to cold, as well • Very uncommon coma & die. • loss of hair • Weight gain
Dental implication • Myxedema coma • Precipitating factor • Trauma , surgery , infection , G.A • Sedative ( diazepam ) analgesic ( codeine ) . The respiratory center is hypersensitive to these drugs , they should be avoided or the dose must be reduced . • Manifestation • Hypothermia , Hypofuntion , Bradycardia , Epileptic seizures • Management • Call ambulance for hospitalization • Artificial respiration • 200 mg hydrocortisone i.v.
Diabetes Mellitus • Definition • It is an endocrine disorder , characterized by persist rise in blood glucose level , • Resulting from absolute or relative deficiency of insulin . Insulin reduces blood sugar level by : - • Glucose oxidation • Glycogensis . • Increase uptake of glucose by cells • Etiology :- • 1- Primary ( idiopathic ) • A- insulin dependent ( juvenile onset ) • B- Non – insulin dependent ( maturity onset ) • 2- Secondary • A- Pancreatic damage ( Chronic pancreatitis , Hemochromatosis . ) • B- Genetic syndrome ( insulin resistance ) • C- Endocrinal ( Acromegaly , Cushing , pheochromocytoma , Steroid therapy )
Comparison of Insulin-Dependent and Non-Insulin Dependent Diabetes Mellitus
Manifestations of diabetes are due to :- • 1- hyperglycemia • 2- Ketoacidosis • 3- vascular wall disease • 4- Advanced glycosylated end products ( AGEs ) • 5- hyperlipidemea • Diagnosis • 1- Glucose tolerance test . • 2- High glycsylated hemoglobin ( reflects blood sugar level in the last 3 months ). If :- • A- < 7% it is normal , patient is not diabetic • B- 7-9 % patient is controlled . • C- > 13 % patient is not controlled . • 3- Ketoacidosis • 4- Glucosuria
Oral manifestations . • No specific pathogonomic features . • More obvious in uncontrolled diabetics . • 1- Dry mouth • 2- Atrophy of filiform papilla & enlarged hyperemic fungiform papillae . • 3- Burning sensation of the tongue . • 4- Periodontal disease ( periodontal abscess in uncontrolled ) • 5- Occasionally enlarged salivary glands . • 6- Increased rate of dental caries . • 7- odontalgia ( due to pulp necrosis ) • 8-Grinspan syndrome : ( it consists of ) • Diabetes • Hypertension • Lichenoid reaction.
Mangement of diabetic patients A- Patient controlled by diet or diet & ant diabetic drugs . • The dentist should reassure the patient to take his meal & ant diabetic drugs • B - Patient controlled by diet & insulin . • These measurements are undertaken for the controlled patient only .but the uncontrolled patient should be to the physician before any dental procedure . • 1- Dental appointment should be in the morning about 1-2 hours after breakfast • And after the usual insulin dose . • 2- Premedication :- sedative or tranqllizer ( to decrease endogenous adrenaline ) • 3- Antibiotic cover when surgery is indicated . • 4- Avoid long appointments . • 5- Avoid excessive trauma during surgical procedure . • 6- Remove all septic foci and maintain good oral hygiene .
7- Local anesthesia :- the lowest concentration of adrenaline ( vasoconstrictor is essential to decrease pain ) or use prilocaine plus octapressin . • 8- G.A ( by anaesthetist ) • 9- Hospitalization ( multiple extraction, massive infection , patient is receiving more than 60 units insulin / day . • 10 – Unconsciousness in dental surgery is frequently due to hypoglycemia . 25 gm glucose orally or 20 ml of 20% dextrose i.v. will relieve hypoglycemia rapidly . • If this is ineffective , call the ambulance .
Effect of low glucose level • Brain use only glucose , if its level falls • 1- neuroglycopenia → irritability , tremor , confusion & loss of concentration . • 2- Adrenaline release → tachycardia , palpation & sweating . • Hypoglycemic shock is more dangerous than hyperglycemic shock because of neuroglycopenia .
A- Jaundice (icterus): Jaundice : excessive bilirubin in the circulation. • Hemolyticjaundice: hemolysis of red blood cells. • Obstructivejaundice: obstruction in the biliary tree: stones, infectious or neoplastic lesions. • Hepatocellularjaundice: liver disease.
Symptoms • Excess of bilirubin. • Color of the skin, oral mucous membrane, and sclera. • Hepatocellular disease: a deficiency of prothrombin and clotting factors. • Decreased tolerance to anesthetics and medications. • History of contact with hepatitis pt. Refer to physician.