Download
1 / 21
210 likes | 242 Views
Explore the impact of 1997 NHIS redesign on childhood asthma prevalence estimates, trends, and implications for public health strategies.

E N D
US Childhood Asthma Prevalence Estimates: The Impact of the 1997 National Health Interview Survey Redesign Lara Akinbami, MD National Center for Health Statistics, Centers for Disease Control and Prevention
Why track asthma prevalence? • High impact on pediatric population • Dramatic increase in prevalence over the past two decades
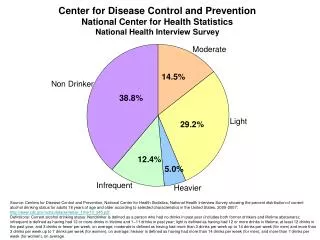
Childhood asthma: definition and impact • Chronic disease with episodic airway inflammation and reactivity that causes airflow obstruction • One of the most common chronic childhood illnesses and a leading cause of disability • 14 million missed school days • Disproportionate use of health care services compared to children without asthma 2.2 times as many ER visits 3.5 times as many hospitalizations • Nearly 200 children die each year
Increasing asthma period prevalence among children 0-17 years of age, 1980-1996 ? Source: National Health Interview Survey, NCHS, CDC
The 1997 redesign of the National Health Interview Survey interrupted monitoring of the asthma period prevalence trend Asthma attack prevalence Asthma period prevalence NHIS redesign Source: National Health Interview Survey, NCHS, CDC
The National Health Interview Survey (NHIS) • Continuous household survey of a representative sample of the US civilian noninstitutionalized population • Face-to-face survey about health conditions and behaviors, including asthma • In 1997, the NHIS was redesigned to improve the survey
NHIS 1997 redesign • Elimination of proxy reporting of health conditions (except for children under age 18 years) • Streamlining data collection on health conditions • The sample is no longer divided between 6 condition lists • Therefore, a larger annual sample of children are asked about asthma • Change in question wording for chronic conditions: doctor diagnosis required
Evaluating the impact of the 1997 NHIS redesign on childhood asthma prevalence estimates • The 1988 NHIS contained the Child Health Supplement (CHS) which included similar questions to those in the 1997 redesigned NHIS • The 1988 NHIS also included the standard asthma question used before 1997 • Allows comparison of estimates obtained from the “old” standard question to those from questions more similar to the new questions
Asthma questions from “old” NHIS, 1988 CHS and redesigned NHIS
Impact of redesign on asthma prevalence estimates on race/ethnicity and age subgroups
Study groups 1 and 2 from 1988 NHIS/CHS Std NHIS • Study Group 1 Responses for standard NHIS asthma question of 1/6 sample (5,509 children) compared to Responses for CHS asthma questions of 1/2 sample (16,624 children) • Study group 2: Responses for standard NHIS asthma question compared to those for CHS asthma questions for 1/12 sample with responses to BOTH CHS and standard NHIS (shown in hatchedarea --2,805 children) sample Child health supplement sample
Differences between standard NHIS and CHS asthma prevalence estimates, 1988 * Relative standard error >30% -- the estimate is unreliable
Calculating inflation factors for the redesigned NHIS estimates • The differences between 1988 CHS and standard NHIS estimates were used to inflate the redesigned NHIS estimates • Method 1 (using study group 1 results) • Method 2 (using study group 2 results) • Two sets of estimates were calculated • Overall asthma period prevalence estimates for 1997-2000 NHIS • Race/ethnicity and age group asthma period prevalence estimates for the 1997-2000 NHIS
Original asthma attack prevalence and modified estimates and 95% confidence intervals, NHIS, children 0–17 years
Asthma period prevalence (1980-1996) and modified asthma attack prevalence estimates (1997–2000), NHIS, children 0–17 years NHIS redesign
Asthma period prevalence (1980-1996), asthma attack prevalence (1997-2003), modified estimates (1997-2000) & current asthma prevalence (2001-2003) NHIS redesign
Summary--general implications • Disease prevalence estimates are sensitive to case definition (caveat—there is no way to know the “true” prevalence) • Surveillance systems using survey instruments may face interrupted trends when surveys undergo periodic revision • Analysis of trends must include examination of underlying data collection methods
Summary—implications for measuring asthma prevalence • The 1997 NHIS redesign interrupted the data trend • The redesigned NHIS measures a different aspect of asthma as reflected in changes in the asthma questions • “Adjusting” 1997-2000 estimates suggests that asthma prevalence plateaued in the mid 1990s • New current asthma prevalence estimates are available beginning in 2001, but these also measure a different aspect of asthma and are not comparable to pre-1997 NHIS estimates
Limitations • Questions from the 1988 CHS and the redesigned NHIS differ • Changes in question ordering not taken into account • Survey weights used to estimate asthma prevalence among study group 2 (1/12th sample) were not designed for this purpose
References 1. Newacheck PW, Halfon N. Prevalence, impact and trends in childhood disability due to asthma. Arch Pediatr Adolesc Med 2000;154: 287-293. 2. Weiss KB, Gergen PJ, Hodgson TA. An economic evaluation of asthma in the United States. N Engl J Med 1992;326:862–6. 3. Centers for Disease Control and Prevention. Asthma Prevalence, Health Care Use and Mortality, 2002. http://www.cdc.gov/nchs/products/pubs/pubd/hestats/asthma/asthma.htm 4. Akinbami LJ, Schoendorf KC. Trends in childhood asthma prevalence, health care utilization, and mortality. Pediatrics 2002;110:315–22. 5. Centers for Disease Control and Prevention. Surveillance for Asthma --- United States, 1980—1999. March 29, 2002 / 51(SS01);1-13. http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5101a1.htm
References 6. National Center for Health Statistics. Health measures in the new 1997 redesigned National Health Interview Survey (NHIS). Hyattsville, MD: National Center for Health Statistics, 2000. (http://www.cdc.gov/nchs/about/major/nhis/hisdesgn.htm). 7. Centers for Disease Control and Prevention. Measuring childhood asthma prevalence before and after the 1997 redesign of the National Health Interview Survey—United States. Morb Mort Wkl Rep October 13, 2000 / 49(40);908-911. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4940a2.htm 8. Akinbami LJ, Schoendorf KC, Parker JD. US Childhood Asthma Prevalence Estimates: The Impact of the 1997 National Health Interview Survey Redesign. Am J Epidemiol 2003;158:99–104.