Burst Abdomen
Burst Abdomen. Presented by Dr. Saifuddin Ahmed. Definition. Post-operative separation of the abdominal musculo-aponeurotic layers. Mean time for dehiscence after 8 to 10 days. . Incidence . Incidence Historical 10%

Burst Abdomen
E N D
Presentation Transcript
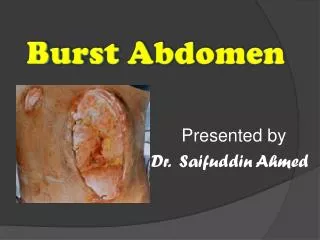
Burst Abdomen Presented by Dr. Saifuddin Ahmed
Definition • Post-operative separation of the abdominal musculo-aponeurotic layers. • Mean time for dehiscence after 8 to 10 days.
Incidence • Incidence • Historical 10% • Recent study – 3.2% [Veterens Affairs Quality programme]
Predisposing factors • 6S • Surgery • Surgeon • Sutures • Sepsis • Straining • Sick patient
Predisposing factors • Surgery • Grossly contaminated surgery • Peritonitis • Biliary-fistula • Faecal-fistula
Predisposing factors • Surgeon • Technique • Meticulous dissection • Haemostasis. • Gentle tissue handling • Tensionless sutures • Incision • Vertical incision worse than Transverse.
Predisposing factors • Straining • Violent cough • Persistent vomiting • Distension • Paralytic ileus • Sepsis • Uncontrolled sepsis
Predisposing factors • Sick patient • Malignancy • Jaundice • Obesity • Anaemia • Hypo-proteinemia • Uremia • Sutures • Prefer non-absorbable sutures
Predisposing factors • Pre-operative • Cough • Anaemia • Hypo-proteinemia • Malnutrition • Steroid
Predisposing factors • Post-operative • Cough • Abdominal distension • Ascitis • Vomiting • Bowel leakage • Wound infection • Haematoma • Uraemia • Jaundice • Electrolyte imbalance
Mortality • Range • 9 to 43 % • Recent study • 16 % • Prevention is the cornerstone • With meticulous surgical technique
Clinically • Pathognomonic feature • Sudden rush of copious serosanguinous discharge for the wound • Large subcutaneous hematoma • Herniated bowel under the skin • Tympanic boggy swelling
Management • Basic principle • Resuture the wound edges • Replace the eviscerated organs • Prevent • recurrent dehiscence • Later development of ventral hernias • As soon as recognized • Protruding viscera - Warm NS bath • cover with large sterile dressing • Shift to OT
Management • When there is Seepage of serosanguinous fluid through a closed abdominal wound, • Remove one or two sutures in the skin and • Explore the wound manually, using a sterile glove. • Look for any separation of the rectus fascia.
Management • Operating room for primary closure. • Wound dehiscence may or may not be associated with intestinal evisceration. • When evisceration is present, the mortality rate is dramatically increased and may reach 30%.
Management • If only very small area of the wound disrupted • That portion alone sutured • If more than half of the incision disrupted • Suture whole wound afresh
Management • Small deficit • Conservative management • Packing with moist sterile dressing • Transverse elastic dressing • Abdominal binder • Avoid strenous activities • Secondary suturing/ natural healing
Management Large deficit: • NG tube • GA • Lift up edges • Reposition of prolapsed bowel • Extract fragments of suture • Freshen the edges • Retention Suture • Strong monofilament non-absorbable • Continuous/ interrupted stitch.
Retension Sutures • Strong monofilament Nylon • Thread through protective rubber tubing • 2.5 cm apart, 2.5 cm from margin. • All layers of the abdomen taken together. • Stitch off after 2 to 4 weeks.
Retension Sutures Advantage • Reduce chance of evisceration. Disadvantage • Pain, discomfort • Types • Internal • External
References GASTROENTEROLOGY 2003;124:1111–1134