Download
1 / 46
530 likes | 1.11k Views
DISORDERS OF LIPID METABOLISM. Department of Laboratory Medicine West China Medical School Sichuan University 李 萍 (LI Ping). 一、 Plasma Lipoprotein 二、 Disorders of Lipoprotein Metabolism 三、 Analysis Assay 四、 Case analysis. 一、 Plasma Lipoprotein. 分类( classification )

E N D
DISORDERS OF LIPID METABOLISM Department of Laboratory Medicine West China Medical School Sichuan University 李 萍 (LI Ping)
一、Plasma Lipoprotein • 二、Disorders of Lipoprotein Metabolism • 三、Analysis Assay • 四、Case analysis
一、Plasma Lipoprotein 分类(classification) 根据化学结构将血浆脂肪分为胆固醇(cholesterol),甘油三酯(triglyceride) ,磷脂(phospholipid)和游离脂肪酸(free lipid)。 • 脂肪在血浆中以脂蛋白型式存在, 所以高脂血症一定是高脂蛋白血症(hyperlipoproteinemia)。
分类(classification) 根据化学结构,脂蛋白电泳或超速离心对血浆脂蛋白进行分类。主要的脂蛋白有高密度脂蛋白(HDL),低密度脂蛋白(LDL),极低密度脂蛋白(VLDL)和乳糜微粒(CM)。血浆脂蛋白分析可有助于明确病因。 超速离心 CM VLDL LDL HDL 电泳 CM 前β-LP β-LP α-LP 胆固醇主要存在于HDL和LDL中,而甘油三酯主要存在于VLDL和乳糜微粒中。不同的基因缺陷可能产生同样的脂蛋白异常,只有通过广泛的家族分析予以鉴别。
The four main lipoproteins and their functions Liporotein Main apoliporoteins Function CM B48,A-I,C-II,E Largest lipoprotein. Synthesized by gut after a meal. Not present in normal fasting plasma. Main carrier of dietary triglyceride VLDL B100,C-II,E Synthesized in the liver. Main carrier of endogenously produced triglyceride LDL B100 Generated from VLDL in the circulation Main carrier of cholesterol HDL A-I,A-II Smallest but most abundant. Protective function. Takes cholesterol from extrahepatic tissues to the liver for excretion
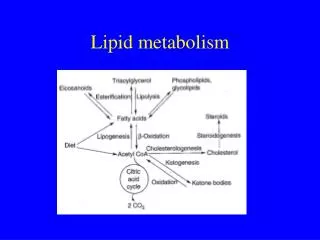
脂蛋白代谢 (Lipoprotein metabolism) 脂蛋白的代谢是以肝脏为中心通过两个循环进行 内源性 外源性 (endogenous) (exogenous) 两个关键酶: 脂蛋白脂酶(Lipoprotein lipase, LPL): 从CM和 VLDL中解离出脂肪酸和甘油至组织 卵磷脂胆固醇酰基转移酶(Lecithin cholesterol acyl transferase, LCAT):使游离胆固醇和脂肪酸形成胆固 醇酯
LDL Receptor Pathway LDL受体途径主要功能:通过摄取胆固醇进入细胞内,用于细胞增殖和类固醇激素及胆汁酸盐的合成等。
Lipoprotein Metabolism (summary) • Lipoprotein are complexes of lipid and proteins which facilitate lipid transport • Their metabolism can be thought of as two interconnected cycles centered on the liver • Lipoproteins are defined by their density and differ in composition, structure and function • Apolipoproteins have a functional as well as structural importance • Cholesterol can only be excreted from the body by way of the liver.
二、Disorders of Lipoprotein Metabolism Lipoprotein disorders are some of the commonest metabolic diseases seen in clinical practice. They may present with their various sequelae which include: • coronary heart disease, CHD • acute pancreatitis • failure to thrive and weakness • cataracts
Classification • Genatic • Pathogeny Primary -- when the disorder is not due to an identifiable underlying disease. Secondary – when the disorder is a manifestation of some other disease.
Primary hyperlipidmias (Fredrickson classfication) • I型高脂蛋白血症(高CM血症) • IIa型高脂蛋白血症(高β脂蛋白血症) • IIb型高脂蛋白血症(高β脂蛋白血症及高前β脂蛋 白血症) • III型高脂蛋白血症(宽β脂蛋白血症) • IV型高脂蛋白血症(高甘油三酯或高VLDL血症) • V型高脂蛋白血症(混合型高脂蛋白血症或高CM和 高VLDL血症)
高脂血症简易分型 分 型 血脂测定 相当于高脂蛋白血症分型 高胆固醇血症 TC IIa 高甘油三酯血症 TG IV(I) 混合型高脂血症 TC、TG IIb(III、V) (括号内为少见类型)
Secondary hyperlipoproteinaemia Two categories • Clinically obvious diseases such as renal failure, nephrotic syndrome and cirrhosis of the liver. • Covert conditions which may present as hyperlipidaemia. These include hypothyroism, diabetes mellitus and alcohol abuse
糖尿病性高脂血症:糖尿病(DM)尤其是非胰岛素依赖性糖尿病(NIDDM)患者常伴有高脂血症。这类患者的血浆脂蛋白改变主要取决于血糖控制情况。糖尿病性高脂血症:糖尿病(DM)尤其是非胰岛素依赖性糖尿病(NIDDM)患者常伴有高脂血症。这类患者的血浆脂蛋白改变主要取决于血糖控制情况。 三种主要表现 1. VLDL CM 疹状黄色瘤 无脂膳食和胰岛素治疗反应良好 (典型的糖尿病性高甘油三酯血症) 2. VLDL 3. VLDL 多见于肥胖
l胰岛素绝对或相对不足,肝脏合成VLDL增加;LPL活性降低,VLDL清除减少。l胰岛素绝对或相对不足,肝脏合成VLDL增加;LPL活性降低,VLDL清除减少。 l糖尿病肾病是影响NIDDM患者血浆脂质水平的另一重要的因素。血浆脂代谢紊乱情况随着肾病的发展及肾衰的加重而恶化。 l肥胖、饮食中高饱和脂肪酸及高胆固醇、缺少运动、 吸烟、饮酒及某些药物也是NIDDM患者血脂异常的 原因。 l脂蛋白糖化影响脂蛋白代谢,LDL的糖化可降低其 与受体的亲和力,导致LDL清除减慢。
甲状腺疾病性高脂血症:甲状腺激素是调节正常生命活动的重要激素。血液中甲状腺激素水平的高低极大地影响着机体的脂质代谢,甲状腺功能降低常伴随脂蛋白代谢异常。甲状腺疾病性高脂血症:甲状腺激素是调节正常生命活动的重要激素。血液中甲状腺激素水平的高低极大地影响着机体的脂质代谢,甲状腺功能降低常伴随脂蛋白代谢异常。 lVLDL和IDL降解减少,使血清LDL水平升高。 l甲状腺激素对胆固醇代谢的双重作用。 l许多甲低患者都伴体重增加。肥胖将成为不依赖甲状腺激素而影响血浆脂蛋白代谢的因素。
肾脏疾病时高脂血症 l肾病综合症:脂代谢紊乱是该综合症的一个重要特点。 TG、TC、VLDL-C和LDL-C均升高, 表现为IIb型。 肾病综合症时的高脂血症是由脂蛋白降解障碍和合成过 多双重机制引起。当尿蛋白量少时,以降解障碍为主, 而当尿蛋白量每天超过10克时,则脂蛋白合成增多成为 主要机制。 l慢性肾功衰:高甘油三酯血症在慢性肾功衰患者中常见。 主要因素是富含甘油三酯的脂蛋白降解减少或组织细胞 对其摄取功能障碍,其次是内源性脂蛋白合成增加。 l急性肾功衰:脂质代谢紊乱特点与慢性肾功衰时相似。
Clinical disorders of lipid metabolism (summary) l The Fredrickson classification is still commonly used to classify hyperlipoproteinaemias by phenotype. lThe genetic and environmental nature of many causes of primary hyperlipidaemia are yet unknown. lSecondary causes of hyperlipidaemia are common and include hypothyroidism, diabetes mellitus, liver disease,renal disease and alcohol abuse.
Management of Hyperlipidaemia The management of hyperlipidaemia is an important aspect of coronary heart disease (CHD) risk factor correction Classification Management Guidelines:NCEP guideline Dietary management:the first line management Drug Therapy
2001年成人治疗计划(ATP III)(美国) 血脂水平的初步分级 (mmol/L) 脂质名称 理想水平 临界水平 异常水平 TC < 5.17 5.17~6.18 6.21 LDL-C < 3.36 3.36~4.11 4.14 HDL-C 1.3 0.91
药物治疗的一般原则 • 降低TC及LDL-C 2001年成人治疗计划 冠心病或其他临床AS疾病 血清LDL-C < 2.6 mmol/L 无冠心病,>= 2 项危险因素 血清LDL-C < 3.38m mol/L 无冠心病,< 2 项危险因素 血清LDL-C < 4. mmol/L • 降低TG及升高HDL-C TG > 11.3 mmol/L 立即治疗 TG 2.3~4.5 mmol/L 应否治疗有争议 TG中度升高,有冠心病及其他危险因素 宜药物治疗 • 特殊人群 老年人 考虑患者的一般健康状况 妇女
高脂血症开始治疗标准值和治疗目标值(mmo/L)(中国)高脂血症开始治疗标准值和治疗目标值(mmo/L)(中国) 饮食疗法开始标准 药物疗法开始标准 治疗目标值 AS病(- ) TC > 5.7 TC > 6.24 TC < 5.72 其他危险因子(- ) LDL-C > 3.64 LDL-C>4.16 LDL-C < 3.64 AS病(- ) TC > 5.20 TC > 5.72 TC < 5.2 其他危险因子(+ ) LDL-C > 3.12 LDL-C>3.64 LDL-C < 3.12 AS病(+ ) TC > 4.68 TC > 5.20 TC < 4.68 LDL-C > 2.60 LDL-C>3.12 LDL-C < 2.60
Management of hyperlipidaemia (summary) • At least two fasting lipid profiles should be performed before starting any form of lipid-lowering therapy • First-line therapy always consists of dietary modification • Drug therapy, if requires, should be viewed as an adjunct to dietary therapy • Other risk factors for coronary heart disease must be managed along with hyperlipidaemia
三、Laboratory analysis 血脂分析不仅对心血管疾病的防治具有重要意义,而且已经渗透并应用于其他诸多临床相关专业疾病的研究,如糖尿病、肾病以及绝经后妇女内分泌代谢改变等
分析前变异对结果的影响 生物学因素(biological factors),如个体间、性别、年龄和种族; 行为因素(behavioral factors),如饮食、肥胖、吸烟、紧张、饮酒、饮咖啡和锻炼等; 临床因素(clinical factors),如 ①疾病诱导(内分泌或代谢性疾病、肾脏疾病、肝脏疾病、贮存性疾病、急性或暂时性疾病等),②药物诱导(抗高血压药,免疫抑制剂性刺激素等); 标本收集与处理,如禁食状态、血液浓缩、抗凝剂与防腐剂、毛细血管与静脉血标本贮存等
NCEP的实验室标准化专家组(LSP)推荐减少血脂和脂蛋白测定分析前因素对结果影响的方法:NCEP的实验室标准化专家组(LSP)推荐减少血脂和脂蛋白测定分析前因素对结果影响的方法: (1)血脂分析前受试者应处于稳定代谢状态; (2)受试者应在血脂分析前至少2周内保持一般饮食 习惯和体重稳定; (3)如血脂检测异常,在作出医学决定以及进一步处 理前,应在两月内进行多次测定,但至少要相隔一周; (4)测定前24h内受试者不应进行剧烈体育运动; (5)禁食或非禁食标本均适用于TC测定,但对于TG和其 他脂蛋白检测需要禁食12h标本;
抽血前受试者至少应坐位休息5min; (7)静脉穿刺过程中止血带使用不应超过1min; (8)血清或血浆标本均适用于TC、TG和HDL-C测定。 如用EDTA作抗凝剂,分离血浆后应立刻放~40C 保存,测定结果乘以1.03后报告; (9)测定TC血清标本可在40C或冰冻进行转送,-200C 贮存标本适于TC测定。但对于TG和其他脂蛋白/ 载脂蛋白测定的标本必须放在-700C或更低温度下 保存; (10)所有血标本应考虑其潜在传染性,应根据有关操 作规程进行处理。
甘油三酯测定 • 化学法:抽提,皂化,氧化,显色 • 甘油激酶法 甘油三酯 脂肪酶 甘油+3脂肪酸 甘油+ATP 甘油激酶 甘油-3-磷酸+ADP 磷酸烯醇式丙酮酸+ADP 丙酮酸激酶 丙酮酸+ATP 丙酮酸+NADH+H+ LDH 乳酸+NAD + 利用340nm光吸收的改变定量甘油三酯 的浓度
胆固醇测定 • 化学法 • 酶法 胆固醇酯+H2O 胆固醇酯酶 胆固醇+脂肪酸 胆固醇+O2 胆固醇氧化酶 胆甾烯酮+H2O2 2H2O2+4-氨基安替比林+酚 过氧化物酶 醌亚胺+4 H2O
血浆脂蛋白测定 • 超速离心法 • 电泳法 • 沉淀分离法 • 遮蔽法 • 变构酶法 • 清除法 载脂蛋白测定
我国血脂异常防治建议和美国NCEP-ATPⅢ规定 临床常规中应至少测定TC、TG、HDL-C 及LDL-C这四项 有条件的地方和实验室条件可测定apoAI、apoB 及Lp(a)
四、Case analysis 病案一 [病史]某男,26岁,其父在35岁时检查出高胆固醇血症并有临床症状, 在39岁时因缺血性心脏病做冠状动脉分流术。姐姐29岁,血浆总胆固醇13.0mmol/L;兄弟22岁,血浆总胆固醇11.3mmol/L。 [体检]符合年轻人外貌,不吸烟,适量饮酒(15个乙醇单位/每周)。未见角膜弓和黄斑瘤,但两手有腱黄瘤,血压16.0/9.3kPa。
[实验室检查] 检验项目 测定结果 参考范围 血浆标本外观 透明 TC(mmol/L) 9.0 3.5~6.5 TG (mmol/L) 1.7 0.5~2.0 HDL-C(mmol/L) 1.27 > 0.9 LDL-C(mmol/L) 6.9 2.0~4.5
血脂变化表 项目入院饮食控制药物治疗停药 TC 9.0 8.3 5.5 8.1mmol/L TG 1.7 1.4 1.3 0.9mmol/L HDL-C 1.27 1.22 1.23 1.21mmol/L LDL-C 6.9 6.4 3.7 6.5mmol/L 问题:可能的诊断是什么?
病案二67岁退休女教师体检发现高脂血症(血浆胆固醇8.6 mmol/L, 甘油三酯 6.6 mmol/L),严格14小时过夜禁食复查,实验室生化检查如下: 初次结果 复查结果 参考范围 Chol 8.6 mmol/L 8.5 3.5~6.2 Trig 6.6 mmol/L 2.1 0.3~1.7 问题: 1.初步诊断是什么? 2. 如何解释初次和复查结果? 3. 进一步需做哪些实验室检查?
实验室肝、肾、甲状腺功能结果 血浆 TP 76 g/L ( 62~82 ) Alb 42 g/L ( 30~50 ) ALT 16 U/L ( < 35 ) ALP 90 U/L ( 30~120 ) Bili 15 umol/L ( < 20 ) T4 16 mmol/L ( 60~160) TSH > 40 U/L ( < 5.5 ) 尿蛋白 < 0.1 g/24h ( < 0.15g/24h)
病案三30岁男性患者外周水肿,实验室生化检查结果如下:病案三30岁男性患者外周水肿,实验室生化检查结果如下: TP 53 g/L (62~82) Alb 25 g/L (30~50) ALT 26 U/L ( < 35 ) ALP 78 U/L (30~120) Bili 10 umol/L ( <20 ) Chol 11.5 mmol/L (< 5.5 ) Trig 1.9 mmol/L (0.3~1.7) 尿蛋白排泄率 8.5 g/24h ( < 1.5 ) 问题:请给出诊断。
病案四The following values are those of an obese 45-year-old man who presented with a myocardial infarct. The lipid studies were performed 8 weeks after recovery. Laboratory results are: Plasma Chol 10.5 mmol/L ( < 5.5 ) Trig 9.5 mmol/L (0.3~1.7) Electrophoresis broad ß-band Comment for this case.
An asymptomatic 38-year-old woman was screened at a well-woman clinic and found to have a non-fasting plasma cholesterol level of 8.7 mmol/l. • What other information and investigations would you require to help in the management of this woman? • What would that management entail? Comment for this case