Download
1 / 45
721 likes | 2.55k Views
Radiology of Caries. ODM 820 spring 2009, May 19 2009. August 2002. August 2005. Introduction. Dental caries is a multifactorial disease with interactions among three factors: the tooth, the microflora , and the diet Caries is an infectious disease since it is the lactic acid

E N D
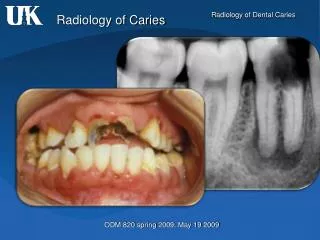
Radiology of Caries ODM 820 spring 2009, May 19 2009
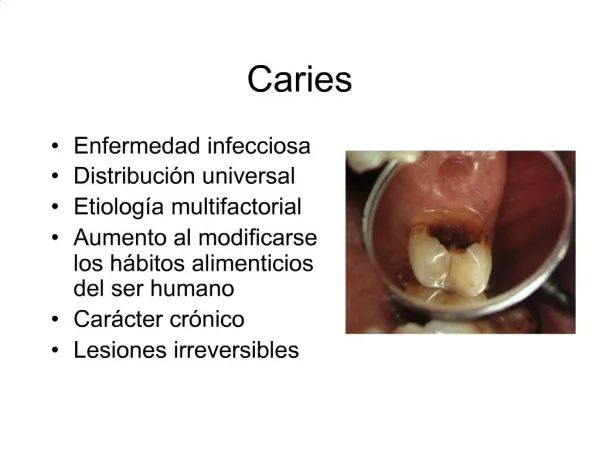
Introduction Dental caries is a multifactorial disease with interactions among three factors: the tooth, the microflora, and the diet Caries is an infectious disease since it is the lactic acid produced by bacteria from the fermentation of the CH that causes the demineralization of the dental hard tissues The initial carious lesion is a subsurface loss of mineral in the outer tooth surface. It appears clinically as a chalky white or an opaque or dark, brownish spot
Use of Intraoral Radiographs Radiography is useful for detecting dental caries because the caries process causes demineralization of enamel and dentin. The lesion is seen in the radiographs as a radiolucent (dark) zone since the demineralized area of the tooth do not absorb as many x-ray photons as the unaffected portion. The radiograph can not detect if the lesion is active or arrested (unless you have different radiographs at different times and you can see the progression of the lesion)
Use of Intraoral Radiographs Radiography is a valuable supplement to a thorough clinical examination of the teeth for detecting caries However, even the most meticulous clinical examination may fail to reveal demineralization beneath the surface, including occlusal surfaces Clinical access to proximal tooth surfaces in contact is limited Several clinical studies have shown that a radiographic examination can reveal carious lesions both in occlusal And proximal surfaces that would otherwise remain undetected
Radiographic examination to detect caries • The BW projection is the most useful radiographic examination for • detecting caries • The use of a film holder with a beam-aiming device reduces the • number of overlapping contact points and improves image quality • Periapical radiographs are useful primarily for detecting changes in the • periapical bone (use of paralleling technique increases the value of • this projection in detecting caries) • Traditionally size 2 “adult” films are used for a BW examination from the • age of 7-8 years onward
Radiographic examination to detect caries • In recent decades there has been a dramatic decline in the prevalence • of caries in all western countries. Accordingly, the interval between • examination should be customized for each individual patient and • based on the perceived caries activity and susceptibility. • Radiographs used to detect carious lesions should be mounted in • frames with dark borders and interpreted using a magnifying glass.
Radiographic detection of lesions • Proximal surfaces • The shape of the early radiolucent lesion in the enamel is classically • a TRIANGLE with its broad base at the tooth surface, spreading • along the enamel rods, but OTHER appearances are common such • as a “band” or a “thin line” • When the demineralization front reaches the dentino-enamel junction • (DEJ), it spreads along the junction, frequently forming the base of • a second TRIANGLE with apex directed towards the pulp chamber. • A lesion of proximal surfaces MOST COMMONLY is found in the area • between the contact point and the free gingival margin. The fact that • the lesion does not start below the gingival margin helps distinguish • a carious lesion from cervical burnout
Radiographic detection of lesions • Classification of the interproximal caries • Incipient Extends less than halfway through the thickness of the • enamel (it is only in enamel !!) • Moderate Extends greater than halfway through the thickness of the • enamel, but does not involve the DEJ • Advanced Extends to the DEJ and into the dentin, but does not • extends through the dentin greater than half the distance • towards the pulp • Severe Extends through the enamel, dentin and greater than • half the distance towards the pulp
Radiographic detection of lesions • Proximal surfaces • Cervical Burnout • Diffuse radiolucent areas with ill defined borders may be apparent • radiographically on the mesial or distal aspects of the teeth in the cervical • regions between the edge of the enamel cap and the crest of the alveolar • ridge cervical burnout This is caused by the normal configuration of the teeth which results in decreased x-ray absorption in the mesial and distal aspects of the teeth
Radiographic detection of lesions • Proximal surfaces • Close attention should be paid to intact proximal surfaces adjacent to • a tooth surface with a restoration since occasionally this surface is • inadvertently damaged during the restorative procedure and is thus • at greater risk for caries • The proximal surfaces of posterior teeth are often broad, the loss of • small amounts of mineral form incipient lesions and the advancing front • of active lesions are often difficult to detect in the radiograph. • Lesions confined to enamel may not be evident radiographicallyuntil • approximately 30% to 40% demineralization has occurred
Radiographic detection of lesions • Proximal surfaces • Even experienced dentist often do not agree on the presence or • absence of caries examining the same set of radiographs, especially • when the lesions are limited to enamel. • A lesions extending into the dentin in the radiograph may be easier • to detect with greater agreement among experienced observers • Potentially, a progressing proximal lesions may be arrested if cavitation • has not developed. If cavitation has occurred, the lesions will always be • active since the bacteria that colonize within the cavity cannot be • removed.
Radiographic detection of lesions • Proximal surfaces Experience !! Caries Detection Years 5 years of practice
Radiographic detection of lesions • Occlusal Surfaces • Carious lesions in children and adolescents most often occur on • occlusal surfaces of posterior teeth. • The demineralization process originates in enamel pits and fissures, • where bacteria plaque can gather. • The lesion spreads along the enamel rods and, if undisturbed, penetrates • to the DEJ, where it may be seen as a thin radiolucent line between • the enamel and the dentin. • Occlusal lesions commonly start in the sides of a fissure wall rather than • at the base and then tend to penetrate nearly perpendicular towards the • DEJ
Radiographic detection of lesions • Occlusal Surfaces • When an occlusal lesion is confined to enamel, the surrounding enamel • often obscures the lesion. As the carious process progresses, a • radiolucent line extends along the DEJ. As the lesions extend into the • dentin, the margin between the carious lesion and non carious dentin is • diffuse. • The classic radiographic appearance of occlusal caries extending into • the dentin is a broad-based, radiolucent zone, often beneath a fissure, • with little or no apparent changes in the enamel
Radiographic detection of lesions • Buccal and Lingual surfaces • Buccal and lingual carious lesions often occur in enamel pits and • fissures of the teeth. When small, these lesions are usually round; as • they enlarge, they become elliptical or semi-lunar. • It is difficult to differentiate between buccal and lingual caries on a • radiograph. When viewing buccal or lingual lesions, the clinician • should look for a uniform non-carious region of enamel surrounding • the apparent radiolucency. • Clinical evaluation is the definitive method
Radiographic detection of lesions • Root surfaces • Root surface lesions involve both cementum and dentin and are • associated with gingival recession. The exposed cementum is relatively • soft and usually only 20 to 50 µm thick near the CEJ, so it rapidly • degrades by attrition, abrasion, and erosion. • Root surface caries should be detected clinically, and often radiographs • are not necessary. • In proximal root surfaces radiographic examination may reveal lesions • that have gone undetected. • Difficult to differentiate between cervical burnout and caries
Radiographic detection of lesions • Associated with dental restorations • A carious lesion developing at the margin of an existing restoration • may be termed secondary or recurrent caries. It should be noted, though, that a lesion developing in a restored surface is mot frequently a new • primary demineralization. • These lesions should be treated like any new caries lesion. • It is important not to confuse secondary caries with residual caries, which • is caries that remain if the original lesion is not completely removed. • A lesion next to a restoration may be obscure by the radiopaque image • of the restoration detection careful examination !!!
Radiographic detection of lesions • Associated with dental restorations • Restorative materials vary in their radiographic appearance depending • on thickness, density, atomic number, and the x-ray beam energy used • to make the radiograph some materials can be confused with caries: • calcium hydroxide is a good example
Enamel caries Recurrent caries Cervical burnout
Recurrent Caries Interproximal caries
Radiographic detection of lesions Interpretation TIPS !! (You will need it) • All films must be properly mounted • Mounted films should be viewed in a room with subdue lighting that is • free of distractions • An illuminator or viewbox is MANDATORY • If the screen of the viewbox is not completely covered by the mounted • radiographs, the harsh light around mounted films must be masked to • reduce glare and intensify the detail and contrast of the radiograph • images • Magnifier mandatory • Use multiples views of the same area
Radiographic detection of lesions Factors influencing caries interpretation • Errors in technique may result in non-diagnostic films. For example, • a BW that is used to detected dental caries must be free of overlapped • contacts. Improper horizontal angulation causes overlapped contact • areas and makes impossible to interpreted the interproximal regions
Radiographic detection of lesions Conditions resembling caries Restorative materials Composites, silicates and acrylics, may resemble caries Careful examination helps to identify the well defined smooth outlines of the preparation
Radiographic detection of lesions Conditions resembling caries Abrasion Abrasion refers to the wearing away of tooth structure from the friction with an foreign object for example tooth brushing On radiographs, tooth abrasion appears as a well defined horizontal radiolucency along the cervical region of a tooth
Radiographic detection of lesions Conditions resembling caries Again…. Cervical Burnout (IMPORTANT) Cervical burnout appears as a collar or wedge- shaped radiolucency on the mesial and distal root surfaces NEAR the CEJ of a tooth May be confused with root caries look at the Alveolar bone level