Download
1 / 37
370 likes | 379 Views
A Socio Cultural Framework for Mental Health and Substance Abuse Service Disparities Research with Multicultural Populations. Margarita Alegria, Ph.D. Glorisa Canino, Ph.D. Harvard Medical School and Cambridge Health Alliance Complexities of Co-Occurring Conditions Conference June 25, 2004.

E N D
A Socio Cultural Framework for Mental Health and Substance Abuse Service Disparities Research with Multicultural Populations Margarita Alegria, Ph.D. Glorisa Canino, Ph.D. Harvard Medical School and Cambridge Health Alliance Complexities of Co-Occurring Conditions Conference June 25, 2004
Acknowledgements Funding for this project was provided by • NIMH -Latino Research Program Project (LRPP) (P01 MH 59876) • NIDA (DA A09438).
Why a Framework for Mental Health and Substance Abuse Service Disparities Research with Multicultural Populations?
Racial and ethnic disparities in health care exist and are associated with worse outcomes, making them unacceptable. Many sources – including health systems, health care providers, patients, and utilization managers – contribute to racial and ethnic disparities in health care.(IOM Report , 2002)That is why we need an approach for reducing racial and ethnic disparities in health care.
Motivation • There are pervasive ethnic and racial disparities in mental health and substance abuse service utilization. Yet the underlying causes of these disparities are poorly understood. The importance of obtaining a clearer understanding of the factors accounting for the ethnic/racial, cultural and contextual differences in sa/mh service utilization is critical due to the rapid growth of ethnic/racial minority populations in the United States (U.S.). Census projections estimate that Latinos will comprise nearly one-fourth of our nation’s population by 2050. The service needs of multicultural populations are of national interest, particularly because of the documented pattern of health care service inequities and potential negative consequences of these inequities for this population.
Racial and ethnic minorities have less access to substance abuse and mental health services than Whites, are less likely to receive needed care and are more likely to receive poor quality care when needed. Higher risk of being misdiagnosed Less likely than whites to receive evidence based Tx Less likely to receive proper medication when first diagnosed
Motivation for Framework • Lacked models to facilitate understanding of mh and substance abuse disparities for ethnic and racial minorities • Evidence of sociocultural and contextual elements having role in service delivery and how minorities interface with services • Interactive and reciprocal dynamics of patient, provider, community and service systems that adds layers of complexity to identifying service disparities • Absence of frameworks to develop public policies, systematic guidelines, training of professional or restructuring of mental health system to be responsive to multicultural populations
How do we define Service Disparities? • Start by expanding IOM’s definition as “racial and ethnic differences in the access, quality and outcomes of health/sa/mh care that are not due to clinical needs, preferences and appropriateness of intervention.” • Difference from IOM’s definition: we postulate 6 rather than 2 sources of service disparities and include rather than exclude access related factors as service disparities factors.
Factors that may influence MH and SA Service Disparities: • The operation of the health care system and provider organization (e.g. structure of incentives and supports for servicing multicultural populations [mcp], diversity in workforce, design of services for mcp, provider burden) • Health care policies and regulations at the state and federal level (e.g. budgetary allocations to serve mcp, state eligibility thresholds for public insurance coverage of mcp, state and federal cost-sharing for attracting diverse work force) and market forces(e.g. # of HMO’s and pharmacies in ethnic/racial minority neighborhoods) • The operation of the community system(e.g. community norms to sa & mh, receptivity to sa & mh services, access to public transportation)
Factors that may influence MH and SA Service Disparities: • Biases, uncertainty and stereotyping in the provider-patient interaction(e.g. statistical discrimination, misdiagnoses, mistrust, lack of therapeutic alliance) • Patient and Family level factors (e.g. health literacy, unrealistic expectations about substance abuse and mental health treatments, lack of adherence to Tx, lack of problem recognition, negative attitudes, stigma) • The changing socio-contextual, cultural, and political forces affecting Multicultural populations
The operation of the health care system and provider organization • The climate and culture of provider organizations-racial minorities as less appealing to service organizations (higher illness severity and prematurely terminating Tx) • Institutional racism • Commitment of allocating providers to minority Medicaid beneficiaries (competing for physician services)
The climate and culture of provider organizations • For example, minorities are described as coming to health care with higher levels of illness severity (Vega and Alegría, 2001) and of prematurely terminating treatment (Sue, 1994). In similar fashion, minority Medicaid managed care beneficiaries are seen as having increased probability for missing appointments (Majeroni et al., 1996) which, in a capitated managed care environment, might make them less attractive for physicians. Recent efforts to weave cultural and linguistic competence requirements in the health care system have been met with concern by medical associations (Flores et al., 2003) because physicians may be required to cover the costs of non-reimbursable interpreter services
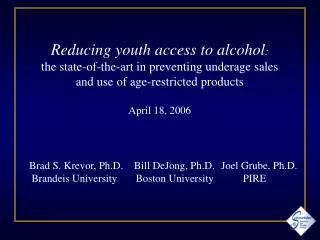
Decreased odds of specialty care use for poor Latinos as compared to poor whites: effect of poverty and minority status (Inequalities in Specialty Care, Alegria et al., Psychiatric Services, 2002 )
TANF/AFDC Medicaid Patients (18 or older) with New Episodes of Depression
Health care policies and regulations at the state and federal level • Organization and financing at state/county level affects access to specialty/substance abuse care • Policies of direct public mh/sa provision of behavioral services • Distribution of HMO’s plans by area • Assurances of geographic distribution of specialty/sa providers • Policies to require in contracts design of targeted services for mcps
Health Care Policies and Regulations at the State and Federal level and Market Forces • For example, state of residence of the child appears to influence the likelihood of receiving mental health/substance abuse care, even after controlling for ethnic and racial differences in the population of children and the level of need (Sturm, Ringel and Andreyeva, 2003). This study found that Latino children had the greatest level of unmet need, and that the states of California, Florida, Texas, Mississippi and Alabama exceeded the national average of unmet mental health/substance abuse need for children 6-17. Geographic differences in mental health/substance abuse care disparities, particularly among children in poor families suggest that state policies and health care market characteristics impact which children get health care. A crucial component seems to be played by State Children’s Health Insurance Programs (SCHIP) designed to make free or low-cost health insurance available to uninsured children not eligible under Medicaid.
Health Care Policies and Regulations at the State and Federal level and Market Forces • The structure of the Medicaid contracts with independent practice associations (IPAs) who service minority Medicaid beneficiaries may also indirectly impact service disparities. Contracts with IPAs that do not include a sufficient pool of providers with language or cultural competencies to service non-English populations, or that do not have practices located near residential areas where ethnic and racial minority enrollees live, may lead to service disparities (Sue et al., 1991).
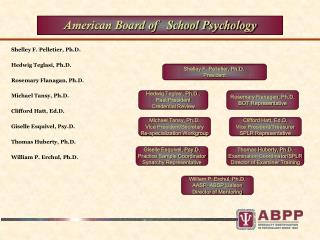
Twelve-Month Rates of Utilization of Health Care Services by Mexican Americans with Mental and Substance Use Disorders Vega WA, et al. Gaps in service utilization by Mexican Americans with mental health problems. Am J Psychiatry 1999;156:928-34.
The changing socio-contextual, cultural, and political forces affecting Multicultural populations • Education • Employment • Housing • Political relationships between country of exit and the US may determine eligibility for government aid and health benefits • Political conditions in the US
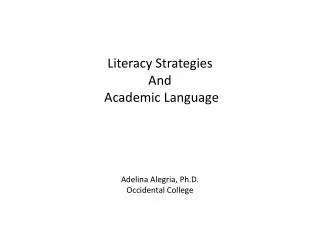
Private Insurance Among Latinos is Decreasing Ruiz P. Issues in the psychiatric care of Hispanics. Psychiatric Services 1997;48:539-40.
The operation of the community system • Support and availability of CBO’s at the neighborhood level • Level of community mistrust in health, sa and mh care providers • Community social and contextual problems that compete for attention (housing, jobs) • Neighbors and extended family’s willingness to intervene-community cohesion • High tolerance for untreated mental illness • Community’s poor perception of the effectiveness of sa and mh care
Community Mistrust in MH/SA Care • Mistrust in Service Providers and Medical Institutions: in NLAAS, about 20% of respondents indicate having negative experience w service providers • Experience that Tx does not help a lot: only 50% rated psychiatric/substance abuse Tx as helping them a lot. • Dropping out of Tx: only 57.14% of respondents in NLAAS say they completed the treatment. • Mode number of visits is 1 and median is 3 to both psychiatrists and psychologists.
Logit Model for Received Active Tx (TANF/AFDC Sample (N=17,772) for those w New Depression
Biases, uncertainty and stereotyping in the provider-patient interaction • Bias by providers in the clinical encounter (e.g. negative attitudes) • Problems in the therapeutic alliance due to stereotyping • Miscommunication in the clinical encounter leading to uncertainty • Bringing past experiences of racist Tx (patient side) or negative experiences w/ minority patients (provider side)
Uncertainty may lead Providers to adopt stereotypes • Cooper’s data in studying patient-provider communication showed that providers may unintentionally incorporate racial and ethnic stereotypes into their interpretations of patients’ symptoms, prediction of patients’ behaviors and medical decision-making. • Short cuts may be necessary given limited exposure or experience w/ particular population.
Unsuccessful Provider-patient Interaction • Studies emphasize that racial and cultural differences between patient and provider may affect the patient’s satisfaction with and continuation in care (Saha, Komaromy, Koepsell et al., 1999). Having a successful interaction between caregiver and clinician has an effect on the degree of resistance or cooperation, the level of disclosure (Chiu, 1994), and the rejection of treatment options (Temkin-Greener and Clark, 1988).
Patient and Family level factors • Low priority to MH/SA Tx • Multiple jobs of minorities and importance of retaining a job • Family and social networks against mh Tx • Limited knowledge of MH/SA and of MH/SA sector, including use of alternative sources (clergy) • Difficulty in communicating need and goals of TX
Patient and Family level factors • Disparities in health care show that some ethnic minority children have also been tied to parental knowledge of available treatments (Bussing, Schoenberg and Perwien, 1998). Bussing and colleagues’ results (1998) reveal significant differences among African American and white parents in their knowledge of attention deficit hyperactivity disorder (ADHD). Only 36% of African American parents reported that they knew some or a lot about ADHD in contrast to 70% of white parents. Recent data suggests that increased parental knowledge about ADHD increases the likelihood of enrollment in both pharmacological treatments and non-pharmacological treatments (Corkunu, Rimer and Schachar, 1999).
Recommended mechanisms to deal w MH/SA Service Disparities • Restructuring of Service Sectors and Changing Recertification of Provider Organizations for Public contracts • Reforming health policies to make them sensitive to needs of mcps • Training and monitoring to avoid stereotypes, prejudice and clinical uncertainty (e.g. cultural liaisons) • Augmenting information exchange between client and provider (more time in clinical encounter, required assessment) for mcp
Recommended mechanisms to deal with MH/SA Service Disparities • Evaluate service procedures to see how can you do better treatment matching (who, when, how) • Increased client/patient activation or empowerment (e.g. RQP) • Review institutional policies in health care systems and implement changes to provider organizations to reduce service disparities • Consider regulating markets • Create annual report card on service disparities at state and county level