Download
1 / 33
340 likes | 435 Views
Rehabilitation Following Brachial Plexopathy “Stingers” . Scott Kaylor, PT, DPT, SCS Proaxis Therapy. Acknowledgements. Timothy McHenry III, MD Whitney Wiles, ATC Matthew Baird, MD Tom Denninger, PT, DPT, OCS, FAAOMPT Chuck Thigpen, PhD, PT, ATC. Objectives.

E N D
Rehabilitation Following Brachial Plexopathy“Stingers” Scott Kaylor, PT, DPT, SCS Proaxis Therapy
Acknowledgements • Timothy McHenry III, MD • Whitney Wiles, ATC • Matthew Baird, MD • Tom Denninger, PT, DPT, OCS, FAAOMPT • Chuck Thigpen, PhD, PT, ATC
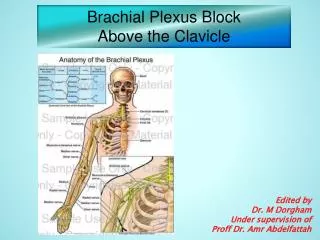
Objectives • To identify the prevalence of brachial plexopathy. • To identify the anatomy involved with brachial plexopathy injury. • To describe an evidence-based return-to-play progression that is criteria driven.
Prevalence and Incidence • Common in contact and collision sports. • Reported annual incidence of a stinger is between 49-65% in collegiate-level football players over a 4-year career • Recurrence rate 57% • 5-10% of players have more serious injuries with prolonged neurological deficits
Signs and Symptoms Common Red Flags Bilateral symptoms or symptoms into more than one limb. Suspect spinal cord involvement If the player remains on the “field of play” the possibility of a spinal cord injury must be considered and ruled out before he is allowed to walk. • Unilateral UE involvement • A traumatic event • Painful sensation that radiates from their neck to their finger tips • Lancinating, burning pain, and dysesthesia usually in a dermatomal pattern. • Weakness/”dead arm”
Symptom Duration • Pain typically seconds to hours. • Rarely beyond 24-hours • May experience weakness in deltoid and supra/infraspinatus that typically resolves in 24-hours to 6 weeks.
Injury Grading • Grade I • neurapraxia • Grade II • axonotmesis • Grade III • neurotmesis
Management Phase 2 Phase 4 Phase I Phase 3
Phase I Rehabilitation • Pain control • Restore cervical ROM • Initial muscle facilitation
Phase I Rehabilitation • Manual Therapy • Traction • Joint mobilization • Soft tissue mobilization • Modalities • Traction • E-stim
Phase I Rehabilitation • 1st Rib Mobilization • Elevated 1st rib due to scalene spasm • Assess with cervical rotation lateral flexion test
Phase I Exercise Examples • Supported chin tucks • With biofeedback
Phase I Rehabilitation • Neural Dynamics • Sliders vs. tensioners to increase excursion • Do NOT want to increase strain during healing
Phase I Rehabilitation • Cervical ROM • Adjust and progress positioning
Criteria to Begin Phase II • Full cervical ROM • Resolution of upper extremity symptoms • Not necessarily full resolution of strength • Be able to maintain a supine chin tuck for 30 seconds
Phase II Rehabilitation • Improve shoulder mobility as needed • Improve muscular endurance • Incorporate extremity movements with stabilization.
Phase II Rehabilitation • Shoulder mobility
Phase II Exercise Examples • Quadruped and prone chin tucks • Cervical stabilization with extremity movements • “No Money” • Dying bug • Half kneel chop and lift • Upper extremity exercises • Bands • PNF • Isotonics
Phase II Exercise Examples • Shoulder Strengthening
Phase II Exercise Examples • Half Kneel Chop and Lift
Criteria to Begin Phase III • Be able to hold chin tuck with head lift (without helmet) for 30 seconds • > 4/5 upper extremity strength to be able to perform light-to-moderate upper extremity strengthening without symptoms
Phase III Rehabilitation • Improve muscular strength • Implement sport specific activities without contact
Phase III Exercise Examples • Cervical Strengthening • Participation in weight lifting with team
Phase IV Rehabilitation • Criteria to begin phase IV • Be able to maintain a chin tuck with head lift wearing a helmet > 30 seconds • No symptoms • Full upper extremity strength
Phase IV Rehabilitation • Phase IV • Initiate contact drills • Percussion to Erb’s Point • Spurling’s Test • Return-to-play
Return to Play Criteria • General RTP Criteria: • Adequate time to heal from primary injury • Absence of underlying conditions that pose undue risk of further injury • Resolution of all symptoms • Full, pain-free ROM • Appropriate cardiovascular fitness • Normal strength • Ability to perform sport-specific skills without symptoms • Same game if complete resolution of symptoms, return-to-baseline ROM and strength profile.
Slow-to-No Symptom Resolution • Communication with and referral to team physician • Further imaging • Radiographs • MRI • CT scan or SPECT scan • EMG study
Prevention • Identifying those at risk • Post-season questionnaire • Proper tackling techniques • Avoid dropping shoulder • Continued eye contact with opposing player should allow for more upright position • High riding shoulder pads to absorb impact • Protective neck rolls • Prevent excessive lateral flexion & extension of neck • NEVER connect straps from helmet to shoulder pads
Brachial Neuropraxia Postseason Questionnaire • Clin J Sport Med. 2012; (22)6
Key Points • Stingers are common and history of stinger increases likelihood of sustaining subsequent stinger. • Use criteria to drive rehabilitation progressions. • Do not return to play if have not returned to baseline. • Communication with sports medicine team is important, particularly in the presence of slowly resolving symptoms.
References • Vaccaro et al. Return to play criteria for the athlete with cervical spine injuries resulting in stinger and transient quadriplegia/paresis. Spine Journal. 2002 Sep-Oct;2(5):351-6. • Castro, F. Stingers, cervical cord neurapraxia, and stenosis. Clin Sports Med22 (2003) 483-492. • Concannon LG, et al. Radiating upper limb pain in the contact sport athlete: an update on transient quadriparesis and stingers. Curr Sports Med Rep. 2012 Jan-Feb;11(1):28-34. • Coppieters MW, Butler DS. Do ‘sliders’ slide and ‘tensioners’ tension? An analysis of neurodynamic techniques and considerations regarding their application. • Coppieters MW, et al. The immediate effects of cervical lateral glide treatment technique in patients with neurogenic cervicobrachial pain. J Orthop Sports Phys Ther. 2003 July;33(7):369-378. • Coppieters MW, et al. Different nerve-gliding exercises induce different magnitudes of median nerve longitudinal excursion: an in vivo study using dynamic ultrasound imaging. J Orthop Sports Phys Ther. 2009 March;39(3):164-171. • Safran MR. Nerve injury about the shoulder in athletes, part 2. AJSM. 2004;32(4):1063-1076. • Editorial. Improving application of neurodynamic (neural tension) testing and treatments: A message to researchers and clinicians. Manual Therapy. 2005;10:175-179. • Weinstein, SM. Assessment and rehabilitation of the athlete with a stinger. Clinics in Sports Medicine. 1998;(17)1:127-135. • Jellad, A, et al. The value of intermittent cervical traction in recent cervical radiculopathy. Annals of Physical and Rehabilitative Medicine. 2009;(52)638-652. • Schenk, R, et al. Inclusion of mechanical diagnosis and therapy (MDT) in the management of cervical radiculopathy: a case report. The Journal of Manual & Manipulative Therapy. 2008;16(1):E2-E8.
Rihn, JA, et al. Cervical spine injuries in American football. Sports Med. 2009;39(9):697-708. • Cantu RV and Canut RC. Current thinking: return to play and transient quadriplegia. Current Sports Medicine Reports. 2005, 4:27-32. • Abdulwahab, SS and Sabbahi, M. Neck retractions, cervical root decompression, and radicular pain. JOSPT. 2000;30(1):4-12. • Gross, AR, et al. Knowledge to action: A challenge for neck pain treatment. JOSPT. 2009;39(5):351-363. • O’Leary, S, et al. Muscle dysfunction in cervical spine pain: implications for assessment and management. JOSPT. 2009;39(5):324-333. • Ghiselli, G, et al. On-the-field evaluation of an athlete with a head or neck injury. Clin Sports Med. 2003;22:445-465. • Olson, DE, et al. Unilateral cervical nerve injuries: brachial plexopathies. Current Sports Medicine Reports. 2007,6:43-49. • Charbonneau, RM, et al. Brachial neuropraxia in Canadian Atlantic University Sport Football Players: What is the incidence of “stingers”? Clin J Sport Med. 2012; 22(6):472-477. • Weinberg, J, et al. Etiology, treatment, and prevention of athletic “stingers”. Clin Sports Med. 2003,21:493-500. • Standaert CJ and Herring SA. Expert opinion and controversies in musculoskeletal and sports medinice: stingers. Arch Phys Med Rehabil. 2009,90:402-406. • Stracciolini A. Cervical burners in the athlete. Pediatr Case Rev. 2003,3:181-188. • Sterling M. (2003) Development of motor dysfunction following whiplash injury. Pain, 103, 65–73. • Jull, G. (2002) A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache. Spine 27(17), 1835–43.