Download
1 / 57
640 likes | 2.4k Views
Gallbladder and Bile Ducts. Chuan Lu Department of Diagnostic Radiology Taishan Medical University. Anatomy. Various Modalities in Biliary Imaging. US MRCP CT ERCP Percutaneous transhepatic cholangiography. Sagittal image of gallbladder. Gallbladder and Bile Ducts.

E N D
Gallbladder and Bile Ducts Chuan Lu Department of Diagnostic Radiology Taishan Medical University
Various Modalities in Biliary Imaging • US • MRCP • CT • ERCP • Percutaneous transhepatic cholangiography
Gallbladder and Bile Ducts • Normal size of gallbladder: 7~9cm in length ; 3~4cm in width; Wall thickness : 2~3mm • Normal size of bile ducts : CBD:≥8mm =dilated right /left intrahepatic duct just to proximal CHD: 2-3mm ;
Transverse image of the liver • right /left intrahepatic duct just to proximal CHD: 2-3mm ;
Common bile duct CBD:≥8mm =dilated
MR • Magnetic resonance imaging is slightly superior to computed tomography in visualization of tumors. The recent addition of magnetic resonance cholangiography allows visualization of both dilated biliary ducts proximal to the tumor and normal-sized extrahepatic ducts distal to the level of occlusion.
MRCP • Magnetic resonance cholangiography (MRCP) images obtained from the newest diagnostic equipment are comparable in quality to those obtained with Endoscopic Retrograde Cholangiopancreatography (ERCP) and percutaneous transhepatic cholangiography. Ductal or intravenous injection of contrast medium is not necessary and the patient is not exposed to irradiation.
The MRCP creates an enhanced MRI and may be adjusted to optimally visualize the biliary and pancreatic ducts. MRCP显示胆系
MRCP MRCP显示胆系
CT Modern multidetector computed tomography is a new diagnostic imaging tool that allows multiplanar reformation. CT cholangiography performed with 64-channel multidetector .CT scanners could provide much more information regarding the biliary tree and its abnormalities.
Imaging Techniques CT scans were obtained on a 64–channel helical CT scanner with the following parameters: • 0.5 seconds per rotation, 5-mm collimation, pitch of 0.984:1, and tube current of 120 kV per 300– 400 mAs. • Transverse 0.625-mm-thick sections were reformatted into thin-section coronal images, maximum- intensity-projection (MIP) images, and volume- rendered (VR) images. • An intravenous drip infusion of 100 mL of meglumine iotroxate (Biliscopin; Schering, Berlin,Germany) is administered for 50 minutes as a biliary contrast agent 40–60 minutes prior to scanning. This biliary agent has been approved in some countries, including Japan, and has been used for tomographic cholangiography.
Anterior (a) and right superior (b) VR images • show the right posterior hepatic duct (arrow in a) draining into the left hepatic duct.
ERCP, MR cholangiopancreatography, ultrasonography (US), and multidetector CT cholangiography each have their own advantages and disadvantages
Advantages and Disadvantages of Various Modalities in Biliary Imaging Modality Advantages Disadvantages ERCP Permits simultaneous biopsy orInvasive, may not be possible due to altered anatomy Treatment following surgery MRCP Noninvasive, no radiation exposureProne to artifact, provides little functional information, difficult to diagnose calcification, difficult to perform in periampullary area US Noninvasive, easily available,Operator dependent, poor demonstration of peripheral no radiation exposureintrahepatic bile ducts, less consistent Multidetector CT cholangiography Information regarding biliaryRadiation exposure, side effects of the biliary agent, kinetics and function available,limited in patients with poor hepatic function high spatial resolution, short scanning time
Cholecystolithiasis • Gallstone with shadowing: high-level intraluminal echoes+ acoustic shadowing(100%diagnostic) • Mobility of the stone by moving the patient during ultrasound scanning
Cholecystolithiasis • Gallstone with shadowing: high-level intraluminal echoes+ acoustic shadowing(100%diagnostic) • Mobility of the stone by moving the patient during ultrasound scanning
Cholecystolithiasis Gallstone with shadowing: high-level intraluminal echoes+ acoustic shadowing(100%diagnostic) Mobility of the stone by moving the patient during ultrasound scanning
Cholecystolithiasis Gallstone with shadowing: high-level intraluminal echoes+ acoustic shadowing(100%diagnostic) Mobility of the stone by moving the patient during ultrasound scanning
Sludge Nonshadowing echogenic homogenerous mass shifting position slowly
False-negative US (5%): • contracted GB, • GB in anomalous/unusual location • small gallstone • gallstone impacted in GB neck/cystic duct, immobile patient • obese patient • extensive RUQ bowel gas
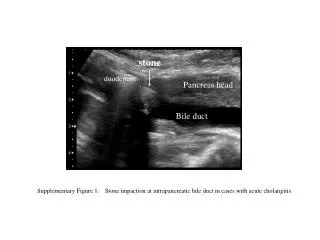
Cholangiolithiasis Stones may develop in the gallbladder and then reflux into the biliary tree to cause focal dilatation of a segment of the biliary tree • Stone visualization in 13-77%(more readily with CBD dilatation+good visibility of pancreatic head) • Dilatation of CBD • Acoustic shadowing • No stone in gallbladder(11%)
Cholangiolithiasis • Stone visualization in 13-77%(more readily with CBD dilatation + good visibility of pancreatic head) • Dilatation of CBD • Acoustic shadowing
Cholangiolithiasis 2 Stone visualization with CBD dilatation
Acute cholecystitis • Wall thickening (over 3mm) and irregularity • Hazy delineation of gallbladder wall • Focal tenderness over gallbladder (sonographic Murphy’s sign) • Cholelithiasis
Acute cholecystitis • Coarse nonshadowing nondependent echodensities= slouged necrotic mucosa/sluge/pus/clotted blood within gallbladder • “halo sign” =GB wall lucency =3 layered configuration with sonolucent middle layer(edema) • Crescent-shaped anechoic pericholecystic fluid • Gallbladder hydrops=distension with AP diameter >5cm
Chronic Cholecystitis • Gallbladder stones • Smooth /irregular GB wall thickening (mean of 5mm) • Mean volume of 42ml
Chronic Cholecystitis • Gallbladder stones • Smooth /irregular GB wall thickening (mean of 5mm) • Mean volume of 42ml
Gallbladder polyp Polypoid / fungating intraluminal mass with wide base
Gallbladder Carcinoma • Associated with: • Disorder of gallbladder: • Cholelithiasis in 64-98% • Gallbladder carcinoma occurs in only 1% of all patients with gallstones! • Porcelain gallbladder (in 4-60%): prevalence of gallbladder carcinoma in 11-22% of autopsies • Chronic cholecystitis • Gallbladder polyp: a polyp >2 cm is likely malignant! • Disorder of bile ducts: • Primary sclerosing cholangitis • Congenital biliary anomalies: cystic dilatation of biliary tree, choledochal cyst, anomalous junction of pancreaticobiliary ducts, low insertion of cystic duct • Inflammatory bowel disease (predominantly ulcerative colitis, less common in Crohn disease) • Familial polyposis coli
Histo: • diffusely infiltrating lesion (68%), • intraluminal polypoid growth (32%) • (a) adenocarcinoma (76%): • (b) rare epithelial cell types: • (c) nonepithelial cell types (2%):carcinoid, carcinosarcoma, basal cell carcinoma, lymphoma
Location • fundus (60%), • body (30%), • neck (10%)
Growth types: • replacement of gallbladder by mass (37-70%) • focal /diffuse irregular asymmetric thickening wall(15-47%) • intraluminal polypoid /fungating intraluminal mass with wide base(14-25%)
Growth types: • pericholecystic infiltration: in 76% focal, in 24% diffuse • dilatation of biliary tree (38 %): • infiltrative tumor growth along cystic duct • lymph node enlargement causing biliary obstruction • intraductal tumor spread • fine granular/punctate flecks of calcification (mucinous adenocarcinoma) • lymph node enlargement in porta hepatis
US: • gallbladder replaced by mass with irregular margins + heterogeneous echotexture (= tumor necrosis) • immobile intraluminal well-defined round/oval mass
Replacement of gallbladder by mass (gallbladder replaced by mass with irregular margins + heterogeneous echotexture (= tumor necrosis)
Cholangiocarcinoma: extrahepatic cholangiocarcinoma=bile duct carcinnoma Growth pattern: • Obstructive type :U/V-shaped obstruction with nipple ,rattail, smooth/ irregular termination • Stenotic type: strictured rigid lumen with irregular margin+ prestenotic dilatation • Polypoid/ papillary type : intraluminal filling defect with irregular margins
A.Extrahepatic tumor(Klatskin’s tumor -tumor located in the hepatic duct bifurcation) B. intrahepatic tumor resulting in biliary duct dilation.
US • Transabdominal ultrasound is a totally painless, non-invasive procedure. The test does not require special preparation, although it is technically easier in patients with at least six hours of fasting. Transabdominal ultrasound is usually recommended as the first imaging modality for the investigation of patients with suspected cholangiocarcinoma. • In hilar cholangiocarcinoma, ultrasound demonstrates bilateral dilation of intrahepatic ducts, and right and left hepatic ducts. • In rare cases, the tumor itself can be visualized as either a hypoechoic (decreased echodensity) or hyperechoic (increased echodensity) rounded mass located just distal to dilated biliary ducts.
Peripheral cholangiocarcinoma may be suspected if abdominal ultrasound demonstrates local dilation of intrahepatic ducts or isolated dilation of the biliary tree inside one lobe of the liver. • In both peripheral and hilar cholangiocarcinoma, biliary ducts distal to the obstruction (common hepatic duct and common bile duct) are not dilated. In patients with hilar cholangiocarcinoma and complete obstruction of both right and left hepatic ducts, extrahepatic bile ducts and the gallbladder appear empty (collapsed) because there is no bile flow out of the liver. • In patients with distal cholangiocarcinoma, ultrasound demonstrates dilated intra- and extrahepatic ducts along with significant dilation of the gallbladder. Peripherally located tumors cause segmental or lobular obstruction of the biliary tree. Bile flow from the rest of the liver is preserved. • Extrahepatic bile ducts and the gallbladder appear normal (filled with bile) in patients with peripheral cholangiocarcinoma.