Download
1 / 32
330 likes | 498 Views
Prevention of osteoporosis in the patient with celiac disease. Harold Rosen, MD Director- Osteoporosis Prevention and Treatment Center Beth Israel Deaconess Medical Center. Potential conflicts of interest. None. Key points- Celiac disease and bone metabolism.

E N D
Prevention of osteoporosis in the patient with celiac disease Harold Rosen, MD Director- Osteoporosis Prevention and Treatment Center Beth Israel Deaconess Medical Center
Key points- Celiac disease and bone metabolism • Vit D/Ca++ deficiency in the general population are common, and result in greater risk of bone loss, fractures, falls, and perhaps infections, autoimmune diseases and cancer. • Patients with malabsorption are at greater risk for D/Ca++ deficiency than most • Patients with celiac disease should be treated with standard doses of calcium (1200 mg) and vitamin D (1000 units) in addition to GFD.
Key points- Celiac disease and bone metabolism (continued) • Since vit D/Ca++ absorption may not completely normalize with GFD, pts with celiac should have adequacy of the vit D/Ca++ regimen checked after 6 months of GFD with measurement of Ca++, alb, phos, Cr, PTH, and 25 OH vit D, in addition to TTG. • We are looking for • nl ca, alb, phos, and cr. • 25 OHD > 20, or 30 ng/ml • PTH <65 (maybe <46)
Key points- Celiac disease and bone metabolism (continued) • The indications for BMD in pts with celiac disease are the same as the indications for BMD in the general population • Men >age 70 • Women > age 65 • (Rosen) – all postmenopausal women
0.5 0.4 0.3 Calcium Absorption Fraction 0.2 0.1 0.0 0 8 16 24 32 40 48 56 64 Serum 25(OH)D, ng/mL 25(OH)D Is Essential for Calcium Absorption Calcium Absorption Plateaus at Serum 25(OH)D Levels 32 ng/mL Bischoff HA et al. J Bone Miner Res. 2003;18:343–351. Heaney RP et al. J Am Coll Nutr. 2003;22:142–146. Barger-Lux MJ et al. J Clin Endocrinol Metab. 2002;87:4952–4956. Adapted from Heaney RP. Am J Clin Nutr. 2004;80(suppl):1706S–1709S. Reproduced with permission form The American Journal of Clinical Nutrition.
LOWESS regression plot of lower extremity function vs vitamin D levels Referencerange 15 Sit-to-stand time, s 14 0 8 16 24 32 40 48 56 64 Serum 25(OH)D, ng/mL Higher 25(OH)D Levels Are Associated With Better Lower Extremity Function Timed Sit-to-Stand Test • 4,100 ambulatory adults included in NHANES III • 60 to 90 years • Functional measurements used to assess lower extremity function: • Timed sit-to-stand test
Fracture risk accdg to 25 OHD levels. Trough at 50 nmol/L, or 20 ng/dl. Melhus et al JCEM 2010; 95:2637
OR for pancreatic cancer in patients according to 25 OHD levels • <10 10-15 15-20 20-30 30-40 >40 • 0.95 0.98 1.04 1.00 1.02 2.12 • Pooled 8 case-control studies, multivariate-adjusted. 95% CI of OR for 25 OHD>40 is 1.23-3.64 American Journal of Epidemiology 2010;172:81
13331 patients from NHANES, cross-sectional study of mortality vs D. Arch Int Med 2008;168:1629
Vitamin D recommendations D amount D levels • IOM 600-800 20-50 • Endocrine Society 1500-2000 30-60 • BIDMC • Low risk patients 1000 don’t check • High risk patients 1500-2000 30-60
Calcium and 800 units of vitamin D for the treatment of osteoporosis NEJM 1992;327:1637 NEJM 1997;337:670
ASBMR 2010, abstract 1163 • Reanalysis of WHI data. • Found that most of the women in the PBO arm (56%) TOOK CALCIUM SUPPLEMENTS OFF PROTOCOL, which would blunt the difference between calcium and PBO. • When you included pts taking no OFF PROTOCOL calcium, risk of heart attack was 21% higher in patients taking calcium and D.
1460 women randomized to 1200 mg of ca vs pbo, followed over 10 yrs.Lewis et al, JBMR 2011;26:35
NEJM 1990;323:878 Women>6 yrs after menopause randomized to 500 mg of calcium vs pbo. In women with baseline calcium intake <400 mg/d, calcium supplements reduced bone loss. In women with calcium intake >400 mg/d, no effect of calcium supplements NEJM 1990;323:878
Calcium conclusions • Estimate dietary calcium intake • 1 serving (300 mg) = • 1 cup of milk, yogurt, beans, collard greens, or almonds • 2 cups of ice cream, cottage cheese, or broccoli • 1 oz of hard cheese • 1 can of sardines or salmon (with bones) • if >1200 mg/d, OK (NEJM 1990;323:878) • Add in supplemental calcium citrate TO GET INTAKE OVER 1200 mg/d • 1000 units of D daily
Citracal’s calcium content is always labelled as per 2 pills! • Preparation Calcium/pill Vitamin D/pill • Citracal+D Caplets 315 250 • Citracal+D 250 250 • Citracal Plus 250 125 • Citracal petites 200 250 • If not enough D, take an extra 1000-2000 units daily. • If that is not enough, consider 50,000 units weekly!
How to put this together? • For patients without particular risk of vitamin D deficiency • 1000 units of vitamin D daily • 1200 mg of TOTAL calcium intake, between diet and supplements • No need to check levels • For patients with high risk of vitamin D deficiency (such as celiac) • 2000 units of vitamin D daily • Verify that 25 OHD levels are 30-60 ng/ml, and adjust dose accordingly
Key points- Celiac disease and bone metabolism (continued) • Since vit D/Ca++ absorption may not completely normalize with GFD, pts with celiac should have adequacy of the vit D/Ca++ regimen checked after 6 months of GFD with measurement of Ca++, alb, phos, Cr, PTH, and 25 OH vit D, in addition to TTG. • We are looking for • nl ca, alb, phos, and cr. • 25 OHD >30 ng/ml (or 40) • PTH <65 (maybe <46)
Ca++ absorption in pts with celiac on GFD 1-12 yrs • Celiacs Controls • Ca++ absorption (%) 39.8(12) 52.3(10) • 25OHD 46(38) 42(21) • Ca++ intake (mg/d) 1129(333) 829(185) • Osteoporosis International 2005;16:56
New NOF GUIDELINES • Screen • women after 65, and men after 70 • >50 if additional risk factors are present • Treat men or women after age 50 if • Vertebral or hip fx, OR • Any T-score <-2.5, OR • T-score –1 to –2.5 and • 10 year hip fracture risk is >3%, http://www.shef.ac.uk/FRAX/
Guide vs guideline • Recall that this is supposed to be a GUIDE (helpful advice), rather than a GUIDELINE (strict rules that must be followed, and if not, punishment ensues). • It is NOT meant to substitute for good clinical judgement: 50 y/o wf with T-score -2.3 and breast cancer on AI, but no other risk factors has a low fracture risk and so does not merit Rx. REALLY?
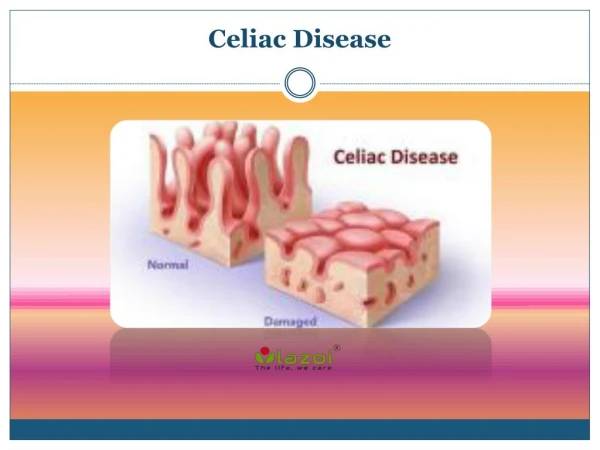
Interpretation of BMD • Osteoporosis – Imminent risk of fracture in the next couple of years, especially if there are pre-existing VCF. All drug trials show a reduction in fracture risk if patients with osteoporosis are treated. Osteopenia – The concern is that with time these patient’s will likely get osteoporosis. No imminent decrease in risk of fracture with treatment, but WE BELIEVE that fracture risk will decrease over time with Rx at menopause. We treat osteopenic women at or after menopause if life expectancy >10 years.
! DO YOU REALLY WANT TO WAIT AND WATCH WHILE THE PICTURE ON THE LEFT TURNS INTO THE PICTURE ON THE RIGHT BEFORE INTERVENING? Normal Bone Osteoporotic Bone
BMD prior to menopause • Not recommended, since we do not recommend treatment for premenopausal women. • Once premenopausal women are treated with enough calcium and vitamin D, BMD should be fairly stable. • No clinical trials of drugs for osteoporosis in premenopausal women have therefore never been done.
Scorecard • Drug abbreviation Brand name class • Alendronate aln Fosamax PO bis • Risedronate ris Actonel PO bis • Ibandronate ibn Boniva PO/IV bis • Zoledronate zol Reclast IV bis • Raloxifene ralox Evista SERM • Calcitonin calc Miacalcin nasal hormone • Denosumab den Prolia ab to RANKL • PTH PTH Forteo anabolic
Guidelines for treatment of osteoporosis • First line – Aln-vs others, longer track record, hip fx efficacy, better BMD data, and cheap generic • Second line – IV zoledronate (better hip fx and BMD data than ralox or ibn) or SQ denosumab • Third line- ralox or ibn • Calcitonin nasal spray has minimal effects on BMD, but may benefit pain slightly • PTH is usually reserved for patients with severe spine osteoporosis, because of best spine BMD data, but cumbersome administration.
Directions for ALN (alendronate) • Take 70 mg once weekly. • Take it first thing in the morning, on an empty stomach, with a full glass of water. • Wait at least ½ hour before eating or lying down. • Put it aside and let us know if you have stomach upset the morning of the ALN.
If intolerant of ALN…. • Reclast (ZOL) can be given as 5 mg once yearly • Side effects can include achiness for a few days after the dose. • One study showed a small increase in atrial fibrillation (1.3% VS 0.5%) • Or • Denosumab (DEN) can be given as 60 mg SQ every 6 months • Side effects include rash (3% vs 1.7% in placebo) and cellulitis (skin infection, 0.3% vs 0.1% in placebo)
Summary • Make sure pts get 1200 mg of calcium (preferrably as citrate) and 1000 units of vitamin D. • If absorption is imperfect, check for 25 OHD>30, PTH <46. Don’t bother checking until patient has been on GFD for 3-6 months • No need for a BMD until menopause. • When drugs indicated, use ALN 70 mg wkly, or if intolerant, IV ZOL 5 mg yearly.