Download
1 / 59
620 likes | 1.15k Views
Modern Treatment of Spinal metastases. Maxwell Boakye , MD MPH FACS FAANS Associate Professor of Neurosurgery Nelson Endowed Chair Center for Advanced Neurosurgery, University of Louisville. My Background. Neurosurgeon Residency 2002

E N D
Modern Treatment of Spinal metastases Maxwell Boakye, MD MPH FACS FAANS Associate Professor of Neurosurgery Nelson Endowed Chair Center for Advanced Neurosurgery, University of Louisville
My Background • Neurosurgeon • Residency 2002 • Fellowships-complex spine-Emory and Spine Oncology-Sloan Kettering-2003 • Stanford-2003-2010-worked with cyberknife • Special interest in spine tumors and spine radiosurgery
Goals • Epidemiology • Presentation • Imaging • Role of Surgery • Emerging Treatment paradigms • Decision making and Frameworks • Memorial Sloan Kettering NOMS criteria • Cases
Epidemiology • 20000 new cases of metastatic epidural cord compression each year • 10% of cancer patients will develop spinal metastatic • About 70% of all cancer deaths occur in elderly patients aged over 65 • Postmortem studies metastases present in 90% of patients with systemic cancer
Epidemiology • Number of elderly patients dying from cancer will double by 2030 • By age 2050, the number of newly diagnosed patients aged 85 will quadruple
Signs and symptoms • Myelopathy-Motor, Sensory, Bowel/Bladder • Usually from epidural cord compression • Pain • Biologic • nocturnal/early morning-resolves during day-usually from tumor infiltration, Steroid responsive • Mechanical-movement related • Radicular-usually epidural disease in foramen • Other Symptoms e.g LOC or AMS from brain
Imaging • X-rays • CT • MRI • PET
Imaging findings • Imaging • Epidural disease only • Vertebral disease only • Vertebral disease with epidural • Cord compression • Mechanical instability • Pathological fractures • Single level, Multiple level, Distant metastases
Treatment options • Surgery • Radiation therapy • Radiosurgery • Chemotherapy
Main surgical approaches • Anterior Transthoracic, Retroperitoneal • Posterior Laminectomy • Posterior transpedicular, costotransversectomy approach
Epidural Compression: Surgery is superior to radiation Patchell et. al, Lancet Vol 366: 643-648, 2005
Surgery improves quality of life outcomes Quan et. Al., Eur Spine Journal 2011 Jun 26
Price of surgery: High Morbidity and mortality • Mortality-5-6% • Complication rates-20-40%
Emerging Treatment Patterns • Vertebral augmentation • Vertebroplasty • Kyphoplasty • Radiosurgery • Combined kyphoplasty and radiosurgery
CYBERKNIFE RADIOSURGERY • The CyberKnife® a robotic manipulator to move a compact linear accelerator with six degrees of freedom • Real-Time Image Guidance Throughout the Treatment • Dynamic Motion Tracking • Allows for accuracy and conformality • Louisville is getting one!!
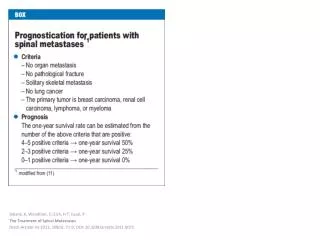
DECISION MAKING • Who should be operated on? • Frameworks for prognosis • Algorithms and Decision aids
Tokuhashi score ≥9:•Excision•Survival > 12 months ≤5:•Palliative•Survival < 3 months
Decision Making-NOMS criteria • Neurologic • Oncologic • Mechanical • Systemic
NOMS criteria • Neurologic-myelopathy, degree of epidural cord compression • Oncologic- radiosensitivity of tumor • Mechanical instability-movement related pain • Systemic disease and medical comorbidities
Neurologic-Classification of epidural compression Bilsky M, Hematol Oncol Clin N Am 20 (2006) 1307–1317
Oncologic-Radiosensitivity • –Myeloma & Lymphoma: most radiosensitive • –Prostate, Breast, Lung and Colon: moderately • –Thyroid, Kidney, Melanoma: not radiosensitive
SINS score • Ranges 0-18 • 0-6, Stable • 7-12, indeterminate, possibly impending instability • 13-18-Instability • Surgical consultation is recommended for SINS score > 7. • Fisher CG, Spine Vol 35(22): 1221-1229, 2010