Understanding Psoriasis: Causes, Symptoms & Treatment Options
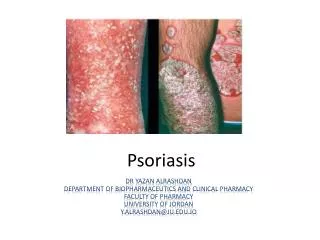
Psoriasis is a chronic inflammatory skin disease affecting 3% of the U.K. population, managed successfully by topical treatments. It has genetic links and unclear inheritance patterns. Infections, medications, alcohol, smoking, climate change, skin trauma, and stress can trigger it. The disease involves epidermal hyperproliferation, accumulation of inflammatory cells, and increased vascularity. Different types like chronic plaque, guttate, flexural, scalp, palmo-plantar, nail, exfoliative erythroderma, acute pustular, and psoriatic arthropathy have varied symptoms and treatment options including medications, UV light, and biologics.

Understanding Psoriasis: Causes, Symptoms & Treatment Options
E N D
Presentation Transcript
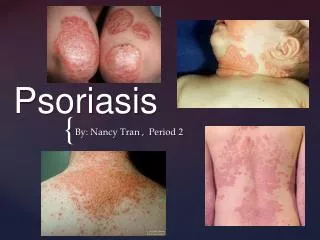
PSORIASIS Kate Blake Lead Nurse Dermatology
Psoriasis • Is a chronic inflammatory skin disease • Affects 3% of U.K. population • 75% are successfully managed in the community with topical treatments (Griffiths,2004) • Also common in India, Far East and parts of Africa
Cause • Strong genetic link • No clear cut inheritance pattern • Poorly understood
Infection Medication Alcohol & Smoking Climate Change Skin Trauma Stress Trigger Factors
Pathology • Epidermal Hyperproliferation • Accumulation of inflammatory cells • Increased vascularity of the upper dermis
Chronic Plaque Psoriasis • Most common • Single or multiple plaques • Red, scaly surface • Vigorous rubbing causes capillary haemorrhage
Chronic Plaque Psoriasis • Predilection for knees, elbows, base of spine • Symmetrical, chronic, & stable • mms to cms in diameter • Sometimes causes itching
Treatment Options • Dithranol / Micanol • Dovonex / Dovobet • Topical steroids • Coal Tar • Ultra Violet Light • Systemics • Biologics
Guttate Psoriasis • Often follows sore throats • Common in young adults • Lesions about 1 cm diameter • Paler pink than established psoriasis • Often resolves rapidly • May enlarge & become stable plaques
Treatment Options • Tar based ointment • Dovonex ; Dovobet • Ultra violet light • Ultra violet light plus tar based ointment • Ultra violet light plus Dovonex
Flexural Psoriasis • May accompany plaque psoriasis • Occurs in groin,natal cleft, axillae & submammary folds • Maceration leaves beefy erythematous rash • Often itchy • Subject to secondary contact sensitivity
Treatment Options • Can be problematic • Mild tar/corticosteroid mixtures may be effective • Steroids can cause striae • Low concentrations of dithranol may burn delicate areas • nUVB & PUVA can be effective if area is accessible
Scalp Psoriasis • Common • Scalp alone may be affected • Lesions very small to whole scalp cover • Occasionally thick and sticks in large chunks to hair • Temporary hair loss
Treatment Options • Tar shampoos • Betamoose • Scalp Blitz • UV combs
Chronic Palmo-plantar Psoriasis • Usually found alone • Erythematous with numerous pustules • Pustules become brown scaly spots & peel off • Painful • Small area or entire surface of palms or soles • May cause considerable disability
Treatment Options • Topical treatments often ineffective • PUVA may give some control • Relapse is common
Nail Psoriasis • Nail involvement frequent • Nail pits • Onycholysis • Can become discolored • Painful • Whole surface may become damaged
Exfoliative Erythroderma • Dermatological emergency • Plaques merge to cover most of skin • Can be slow or rapid • Systemic/ topical steroids may precipitate
Acute Pustular Psoriasis • Dermatological emergency • With or without pre existing psoriasis • Sudden development of widespread erythema • Pustules are sterile • May coalesce to form lakes of pus • High swinging temperature and unwell • Patient may die from secondary infection
Psoriatic Arthropathy • Affects up to 10% of people with psoriasis • Is erosive and may result in joint destruction