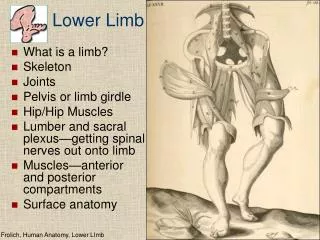
Limb Development
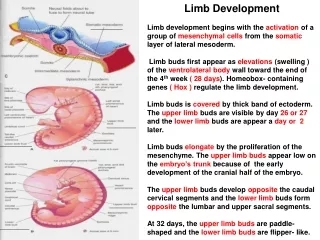
Limb Development Limb development begins with the activation of a group of mesenchymal cells from the somatic layer of lateral mesoderm.

Limb Development
E N D
Presentation Transcript
Limb Development Limb development begins with the activation of a group of mesenchymal cells from the somatic layer of lateral mesoderm. Limb buds first appear as elevations (swelling ) of the ventrolateral body wall toward the end of the 4th week ( 28 days). Homeobox- containing genes ( Hox ) regulate the limb development. Limb buds is covered by thick band of ectoderm. The upper limb buds are visible by day 26 or 27 and the lower limb buds are appear a day or 2 later. Limb buds elongate by the proliferation of the mesenchyme. The upper limb buds appear low on the embryo’s trunk because of the early development of the cranial half of the embryo. The upper limb buds develop opposite the caudal cervical segments and the lower limb buds form opposite the lumbar and upper sacral segments. At 32 days, the upper limb buds are paddle-shaped and the lower limb buds are flipper- like.
At the apex of each limb bud the ectoderm thickens to form an apical ectodermal ridge ( AER ). This ridge exerts an inductive influence on the limb mesenchyme to initiates growth and development of limbs in a proximal- distal axis. Mesenchymal cells aggregate the posterior margin of the limb to form the zone ofpolarizing activity ( ZPA ). Fibroblast growth factors from the AER activate the ZPA
The distal ends of the flipper- like limb buds flatten into paddle- like hand and foot plates. By the end of the 6th week, mesenchymal tissue in the hand plates has condensed to form digital rays. The intervals between the digital rays are occupied by loose mesenchyme. These mesenchyme break down forming notches between the digital rays.
During the 7th week, similar condensations of mesenchyme form digital rays and toe buds in the foot plates. As the tissue breakdown progresses, separate digits are formed by the end of 8th week. Programmed cell death ( apoptosis ) is responsible for tissue breakdown in the interdigital regions and is mediated by bone morphogenetic proteins.
At the tip of each digital ray, a part of the apical ectodermal ridge (AER ) induces development of the mesenchyme into the mesencymal primordia of the bones ( phalanges ) in the digits
Blocking of cellular and molecular apoptosis could account for syndactyly , webbing or fusion of the fingers or toes.
In most bones like the long bones in the limbs, the condensed mesenchyme which develops from mesoderm and neural crest undergoes chondrificaion to form hyaline cartilage bone models. Chondrification centers appear later in the 5th week. By the end of the 6th week, the entire limb skeleton is cartilaginous.
From the dermomyotome regions of the somites, myogenic precursor cells migrate into the limb bud and later differentiate into myoblasts ( precursors of muscle cells ). As the long bones form, myoblasts aggregate and form a large musclemass in each limb bud. In general this muscle mass separates into dorsal ( extensor ) and ventral ( flexor ) components. The mesenchyme in the limb bud gives rise to bone, ligaments and blood vessels. The cervical and lumbosacral myotome contribute to the muscles of the pectoral and pelvic girdles.
Cutaneous Innervation of Limbs Motor axons arising from the spinal cord enter the limb buds during the 5th week and grow into the dorsal and ventral muscle masses. Sensory axons enter the limb buds after the motor and use them for guidance. Neural crest cells ( precursors of Schwann cells ) surround the motor and sensory nerve fibers in the limbs and form the neurolemmal and myelin sheaths.
A dermatome is the area of skin supplied by a single spinal nerve and its ganglion. A cutaneous nerve area is the area of skin supplied by a peripheral nerve. During the 5th week, the peripheral nerves grow from the developing limb plexuses ( brachial and lumbosacral ) into the mesenchyme of the limb buds . The spinal nerves are distributed in segmental bands supplying both dorsal and ventral surfaces of the limb buds. Although the original dermatomal pattern changes during growth of the limbs, the distribution can still be recognized in the adult. In the upper limb, observe that the area supplied by C5 and C6 adjoin the areas supplied by T2, T1 and C8 but the overlap between them is minimal at the ventral axial line.
Originally the flexor aspect of the limbs is ventral and the extensor aspect dorsal and the preaxial and postaxial borders are cranial and caudal respectively.
Early in the 7th week the limbs extend ventrally. The developing upper and lower limbs rotate in opposite directions and to different degrees. The upper limbs rotate laterally 90 degrees on their longitudinal axes. So, the future elbows point dorsally and the extensor muscle lie on the lateral and posterior aspects of the limb. The lower limbs rotate medially through 90 degrees. So, the future knees face ventrally and the extensor muscles lie on the anterior aspect of the lower limb.
Embryo about 52 days. The fingers are separated and the toes are beginning to separate. Note that the feet are fan- shaped. Embryo about 56 days. All regions of the limbs are apparent and the digits in the hands and feet are separated. It should now be clear that the radius & tibia ; ulna & fibula and thumb & great toe are homologous digits.
Joints They develop from interzonal mesenchyme between the primordia of bones. In a fibrous joint the intervening mesenchyme differentiates into dense fibrous connective tissue. In a cartilagenous joint the mesenchyme between the bones differentiates into cartilage. In a synovial joint, a synovial cavity is formed within the intervening mesenchyme by breakdown of the cells. The mesenchyme gives rise to the synovial membrane and the capsular and other ligaments of the joint.
Blood supply to limbs The limb buds are supplied by branches of the dorsal intersegmental arteries which arise from the aorta and form a fine capillary network throughout the mesenchyme. The primordial vascular pattern consists of a primary axial artery and its branches which drain into a peripheral marginal sinus. The primary axial artery becomes the brachial artery in the arm and the common interosseous artery in the forearm which has anterior and posterior interosseous branches. The ulnar and radial arteries are terminal branches of the brachial artery. As the digits form, the marginal sinus breaks up and final venous pattern is represented by basilic and cephalic veins and their tributaries develop. Blood in the marginal sinus drains into a peripheral vein.
In the thigh, the primary axial artery is represented by the deep artery of the thigh ( profunda femoris ). In the leg, the primary axial artery is represented by the anterior and posterior tibial arteries.
Exposure to thalidomide before 33 day may cause The most critical period of limb development is from 24 to 36 days after fertilization. Thalidomide is absolutely contraindicated in women of childbearing age. This drug is used as a sedative and antinauseant. It is a potent human teratogen during the embryonic period.
Major limb anomalies appear about 2 in1000 newborns. Most are caused by genetic factors. Molecular have implicated gene mutation ( Hox gene ) in some cases of limb defects. Several congenital anomalies of arterial pattern may be found in these defects.
Congenital Clubfoot Any deformity of the foot involving the talus ( heel ) is called clubfoot or talipes. It is uncommon, occurring about once in 1000 births. As the children develop, they tends to walk on the ankle ( talus ) rather than on the sole of the foot. Talipes equinovarus, the most common type of clubfoot. It occurs twice in males. The sole is turned medially ( inverted foot ) with hyperextension and incurving of the feet. It results from abnormal positioning or restricted movement of the fetus’s lower limbs in utero. Hereditary factors and environmental factors are involved in most cases. Clubfoot appears to follow a multifactorial pattern of inheritance ( interaction of genetic and environmental factors ).
Development of Appendicular Skeleton It consists of the pectoral and pelvic girdles and limb bones. The model of pectoral girdle and upper limb bones appear slightly before those of the pelvic girdle and lower limbs. The clavicle initially develops by intramembranous ossification and it later forms growth cartilages at both ends. The clavicles begin to ossify before any other bone in the body. The femora are the next bones to show traces of ossification Ossification begins in the long bones by the 8th week of embryonic development and initially occurs in the diaphyses of the bones from primary centers of ossification. By 12 weeks primary ossification centers have appeared in nearly all bones of the limbs.
The first indication of ossification in the cartilaginous model of a long bone is visible near the center of the future shaft ( primary center of ossification ). The part of a bone ossified from a primary center is the diaphysis Primary centers appear at different times in different bones. Most ofthese centers appear between the 7th and 12th weeks of development. All primary centers of ossification are present at birth.
The part of a bone ossified from a secondary center is the epiphysis. The epiphysial plate ( cartilage ) intervenes between the diaphysis and the epiphysis. This plate is response for lengthening of the bone until the final size is reached. The epiphysial plate is replaced by bone development on each of its 2 sides. When this occurs growth of bone ceases. The secondary ossification centers of the bones at the knee are the first to appear. The centers for the distal end of the femur and the proximal end of the tibia appear during the last month of intrauterine life. Most secondary centers of ossification appear after birth.