Brainstem death
Brainstem death. Paulus Anam Ong Department of Neurology. Foreword. The purpose of medical science is to prolong life and not to prolong dying process. Physician:health provider who are authorized to define death of the individual

Brainstem death
E N D
Presentation Transcript
Brainstem death Paulus Anam Ong Department of Neurology
Foreword • The purpose of medical science is to prolong life and not to prolong dying process. • Physician:health provider who are authorized to define death of the individual • Physician should know the definition of death in both emergency or normal situation
Definition of Death • Irreversible loss of the capacity for consciousness, combined with the irreversible loss of the capacity to breath” • The irreversible cessation of brainstem function (brainstem death), whether induced by intracranial events or result of extra-cranial phenomena will produce the same clinical state • Brainstem death is equivalent to death of the individual. U.K. Criteria for the diagnosis of brainstem death (Working Group convened by the Royal Collage of Surgeons, 1995)
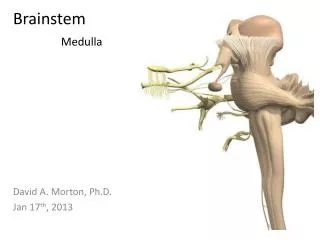
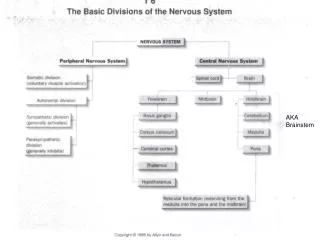
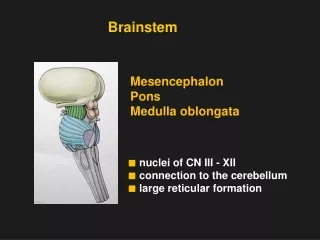
Brainstem death • Brainstem: regulator of respiration and cardiovascular stabilization • Brainstem death: discontinuity of peripheral neuronal system through the brain (absolute for consciousness) • Brainstem death: self-fulfilling prophecy
Diagnosis of Brainstem death 3 step in clinical diagnose of brainstem death: • To ascertain that essential condition be satisfied before considering the diagnosis of brainstem death • Exclude the possibilities of reversible cause of coma and apnea • To ascertain the irreversible absence of brainstem reflexes and the apnea
Ad 1. Certain condition should be satisfied Two Condition required for brainstem death: • The patient is deeply comatose and apnea; unresponsiveness and maintained on the ventilator • The diagnosis should be known and the condition should be one that is capable of causing neuronal death and the brain damage is irreversible
Ad 2. To exclude the reversible cause of comatose and apnea • Drug intoxication (depressant drugs) • Primary hypothermia • Potential metabolic and endocrine disturbances as a cause of comatose • U.K Code: Diagnosis of brainstem death should not be consider with the presence of above points
Before test the brainstem reflexes There should be evidence of loss of brainstem function • Patient is in deeply comatose • There is not abnormal postures (de-cortication or de-cerebration) • There is no occulocephalic reflex • There is no epileptic seizure • There is no spontaneous breath Brainstem is still functioning if one of the above point is present.
5 Brainstem reflexes Absence of : • Pupils: no response to light • Cornea: no corneal reflexes • Oculocephalic testing (head turning) and Oculovestibular (caloric) testing • Motor response to adequate somatic stimulation within distribution of cranial nerve • Gag reflex (pharingeal and tracheal reflexes)
Apnea Test • Prerequisites: • Core temperature >36.5 ‘C • Systolic BP > 90 mmHg • Euvolemia. Option: positive fluid balance in previous 6 h. • Normal Pco2 > 40 mmHg • Normal Po2. Option: preoxigenation to obtain arterial P o2 > 200mmHg • Connect a pulse oximeter and discontect the ventilator
Apnea Test • Deliver 100% O2 6l/min into trachea. • Look closely for respiratory movement (abdominal or chest excursions that produce adequate tidal volumes) • Measure arterial P o2, Pco2 and pH after approximately 8 min and reconnect the ventilar. • If respiratory movement are absent and arterial Pco2 is >60mmHg; the apnea test is (+) support brainstem death • If respiratory movement are observed apnea test is (-) • Connect the ventilator if during testing systolic BP <90mmHg, or cardiac arrythmia or oxygen desaturation are present; immidiately analyze arterial blood gases. If Pco2 is >60 mmHg or Pco2 rise >20mmHg apnea test (+) support brainstem death; if Pco2 is <60mmHg or Pco2 is <20mmHg over baseline, the result is indeterminate, additional confirmatory test can be considered.
Repeat of test • Test repeating is done to avoid fault observation and changes of signs • Interval time of 2 tests range from 25 minutes to 24 hrs depend on hospital regulation and recommendation accepted
Difficulties in diagnosing brainstem death • Severe facial trauma • Disease of pupils • Sedative drug used • Severe pulmonary disease
After diagnosis of brainstem death • Withdraw therapeutic and palliative treatment gradually according to severity of individual patient
Doubt in: • Primary diagnosis • Cause of brainstem dysfunction may be reversible (drug and metabolic disorders) • Completeness of clinical test • Do not make diagnosis of brainstem death
Ancillary Testing No required • USG doppler • MRI • Brainstem Evoke Potential • Electroencephalography
According to Indonesia Doctor Association (IDI) • Diagnosis of brainstem death should be made by at least 2 doctor who are experience in this field • In IndonesiaAnestesiologist, Critical care doctors, Neurologist and both of them do not involved in the organ transplant team