Download
1 / 29
290 likes | 312 Views
Explore the role of laparoscopy in detecting and staging pancreatic cancer, including limitations, peritoneal cytology, factors affecting usefulness, and a cost-benefit analysis.

E N D
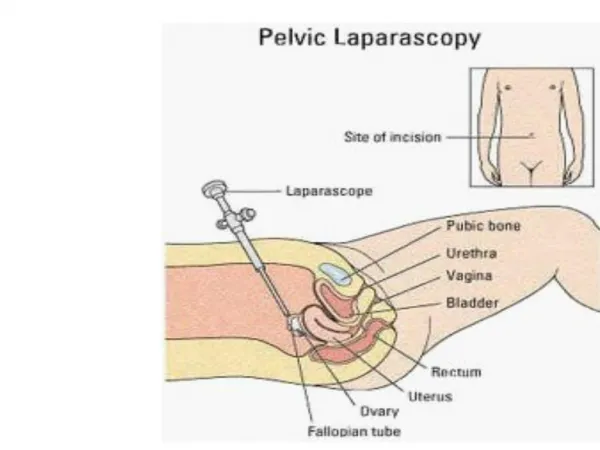
Diagnostic Laparoscopy for Carcinoma of Pancreas Dr. David KK Tsui Department of Surgery Pamela Youde Nethersole Eastern Hospital Hong Kong SAR 15 January 2005 Joint Hospital Surgical Grand Round
1970s & 1980s • Reports from 1970s & 1980s showed the role of laparoscopy in detecting occult metastases, allowing biopsy and avoiding unnecessary laparotomy close to 30 % in Ca pancreas. • But no satisfactory imagings were available during that period of time and a lot of advanced cases were included in their studies Cushieri A et al, Gut 1978 Ishida H et al, Gastrointest Endosc 1983
Obvious carcinomatosis on laparoscopy and it should not be missed on pre-op. CT
1990s • Staging laparoscopy has a sensitivity of 60 - 100% and the incidence of metastases at laparoscopy ranges widely from 14 % to 75 % Catheline JM et al, Chirurgie 1998 Van Dijkum EJMN et al, J AM Coll Surg 1999 John TG et al, World J Surg 1999
What is the true benefit from diagnostic laparoscopy nowadays? • Should we adopt and routine laparoscopy for all the cases?
Limitations of Laparoscopy • Require general anaesthesia • Prior dissection required for patients with previous surgery • Increased operative time requirements and equipment costs • Limited ability to detect retroperitoneal pathologies • Lack of tactile feedback
Laparoscopic USG Laparoscopy with lap USG in Staging of CA pancreas Pisters et al, Br J Surg 2001
Peritoneal Cytology • Can be easily performed during laparoscopy by infusion of 250 – 300 ml normal saline • 33% of positive peritoneal cytology in periampullary carcinoma was found in some series and the yield is related to any pre-operative biopsy Bonenkamp JJ et al, Br J surg 1996 Rubeiro UJ et al, Surg Laparosc Endosc 1998 Warshaw AL et al, AM J Surg 1991
Factors Affecting the Usefulness of Laparoscopy • Pre Operative Imaging • Resectability • Palliation strategy (surgical versus non-surgical) • Tumour Location • Cost-benefit consideration
Pre Operative Imaging • More reliable of “radiographic resectability rate” as a result of improved CT quality, close to 91 % in Memorial Sloan Kettering Cancer Centre Conlon KC et al Ann Surg 1996 Incidence of occult peritoneal or liver metastasis found after helical CT Pisters PWT et al, Br J Surg 2001
Very impressive CT gives you clear image regarding the tumour-vessel relationship
Resectability • “Resectability” would also vary according to different practice and the type of R resection of the study. The exact pathology and the clearance of tumour are not often mentioned in the those studies evaluating the usefulness of laparoscopy Pisters PWT et al, Br J Surg 2001 R0 - gross and microscopic clear R1 - gross clear by microscopic positive margin R2 - both gross and microscopic margin involved
Resectability Overall and Ro Resection Rates Pisters PWT et al, Br J Surg 2001
Palliation Strategy • Obstructive jaundice is the main symptom and this can be effectively achieved by endoscopy and interventional radiology (surgical vs non-surgical strategy) Endoscopic guide Stent insertion Biliary Bypass Surgery – Laparoscopic
Endoscopic Metallic Stenting to relieve biliary obstruction Carcinoma of pancreas with SMV invasion relieved by metallic stent
Gastric Outflow Obstruction Carcinoma of body of pancreas causing GOO
Laparoscopic Gastrojejunostomy Laparoscopic GJ to relieve gastric outflow obstruction
Tumor Location • 28 out of 171 cases (16.4%) of periampullary carcinoma were found to have metastatic deposits on laparotomy, whereas 9 of 17 cases (52.9%) of pancreatic body and tail were having metastatic deposits Barreiro CF et al, J Gastrointest Surg 2002
Tumor Location Vollmer CM et al, Ann Surg 2002
Cost-Benefit Consideration • Routine diagnostic laparoscopy would need to be seven times cheaper than laparotomy to be justifiable from a cost-effective standpoint • However diagnostic laparoscopy costs half as much as diagnostic laparotomy, and therefore routine diagnostic laparoscopy could be recommended • It is not cost effective to use laparoscopy as an alternative to high-quality in a patient who is referred with marginal-quality CT that demonstrate a “resectable” pancreatic tumour Friess H et al J, Am Coll Surg 1998 Pisters PWT et al, Br J Surg 2001
Treatment Algorithm • Obtain preoperative imaging, preferably high-quality CT • Review for radiological resectability in multidisplinary session • Explore options for palliation considering available expertise and patient’s condition • Proceed to surgery
Routine vs Selective Policy • Routine diagnostic laparoscopy should not be considered in obviously metastatic disease • It should not be used to replace high quality CT scan • In view of the cost consideration, indication would depend on how frequent will unnecessary laparotomy be spared. Potter MW et al, Surg Oncol 2000
Conclusion • Diagnostic Laparoscopy for patients with Pancreatic Tumor optimizes patient selection for tumour resection with curative intent • Selective use of Laparoscopy after reviewing the Pre Op Imagings can avoid unnecessary laparotomy • It is particular pronounced when non-surgical palliation is available • Ampulla tumor are almost always resectable