Download
1 / 22
220 likes | 372 Views
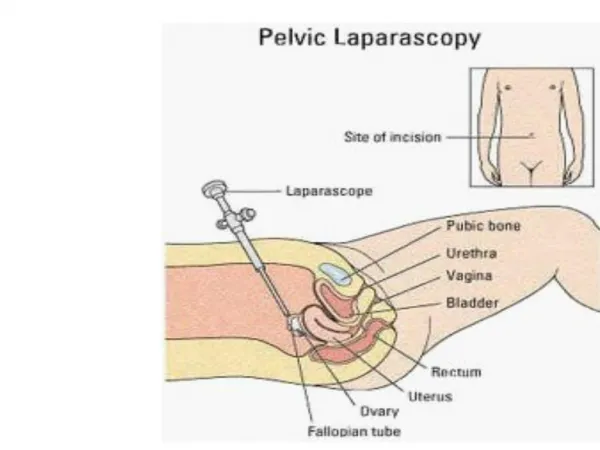
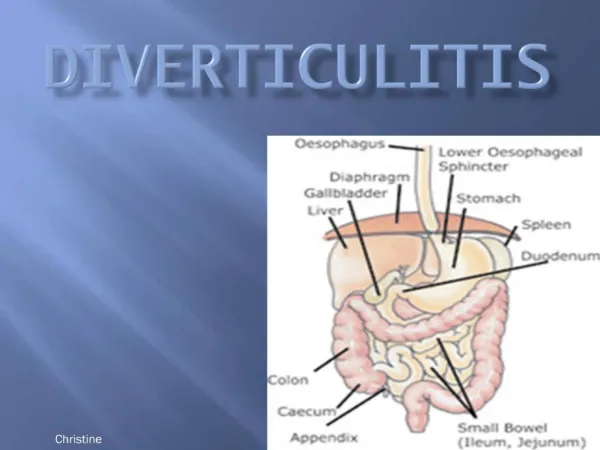
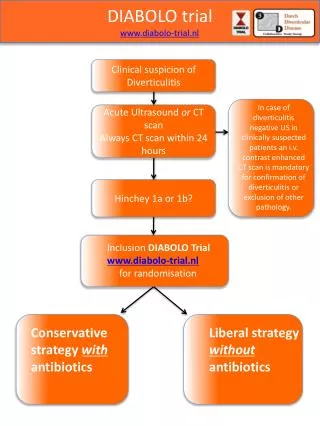
Advantages of Laparoscopy for Diverticulitis. Steven D. Wexner, M.D., FACS, FRCS, FRCS (Ed) Cleveland Clinic Florida Chairman, Department of Colorectal Surgery Chief of Staff, Cleveland Clinic Florida

E N D
Advantages of Laparoscopy for Diverticulitis Steven D. Wexner, M.D., FACS, FRCS, FRCS (Ed) Cleveland Clinic Florida Chairman, Department of Colorectal Surgery Chief of Staff, Cleveland Clinic Florida Professor of Surgery, Ohio State University Health Sciences Center at the Cleveland Clinic Foundation Clinical Professor of Surgery, University of South Florida College of Medicine
Advantages of Laparoscopy: Diverticulitis • Advantages • Operative time • Morbidity • Hospital Length of Stay • Special considerations • Presence of complications • Conversion • Advantages for elderly • Advantages for obese • Cost
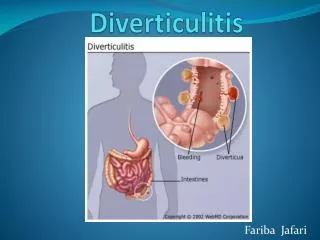
Modified Hinchey* Grading System I. Pericolic abscess IIA. Distant abscess amenable to percutaneous drainage IIB. Complex abscess associated with fistula III. Generalized purulent peritonitis IV. Fecal peritonitis *Adv Surg 1978
Case-Controlled Series *p<0.05 **p<0.001 Advantages of less morbidity and shorter hospitalization
Laparoscopy: DiverticulitisRetrospective/prospective results – Hospital Stay
Laparoscopy: Diverticulitis Retrospective/Prospective Results - Morbidity The more complicated the diverticular disease, the tendency for higher morbidity and longer lengths of hospital stay *p<0.001 **p<0.05
Laparoscopy: Diverticulitis - Comparative Studies *p<0.05 **p<0.001
Laparoscopy: Diverticulitis • 1/95-1/98: 1118 patients • Laparoscopic colorectal surgery study group • 509 sigmoid colectomies • 304 diverticulitis • 249 (81.9%) • Peridiverticulitis • Recurrent inflammation • Stenosis • 26 Hinchey I • 9 Hinchey II • 2 Hinchey III Köckerling et al., Surg Endosc 1999
Laparoscopy: Diverticulitis Stage Conversion Mean operative time Morbidity (n (%)) (min (range)) (%) Total 22/304 (7.2) 164 (65-410) 17 Chronic 12/249 (4.8) 159 (65-395) 14.8 Hinchey I-IV 10/55 (18.2) 182 (90-410) 28.9 I 8/26 (30.7) 183 (100-410) 33.3 II 1/9 (11.1) 198 (90-320) 37.5 III/IV 0/2 (0) 110 (100-120) 50 Köckerling et al., Surg Endosc 1999
Mean age, 59.5 years Mean age, 69.5 years Mean age, 67.9 years Mean age, 54.3 years Mean age, 65.9 years Mean age, 67.7 years Laparoscopy: DiverticulitisComparative Study n = 18 # patients Sher et al, Surg Endosc. 1997
Laparoscopy: Diverticulitis - Comparative Studies Morbidity Morbidity (%) 43 29* 29 13 0 0 Hinchey IIAand IIB OverallLate experience experience * P<0.05 Sher et al, Surg Endosc. 1997
10† 9* 7* 5 5 Laparoscopy: Diverticulitis Open vs. LaparoscopyHospital stay Days * p<0.05 †p<0.01 Sher et al, Surg Endosc. 1997
Open vs. Laparoscopy *p<0.05 **p<0.001
Laparoscopy: Elderly Laparoscopic Open p value n= 22 n = 24 Mean age (yrs) 77.2 (75-82) 78 (76-84) NS Gender (M:F) 10:12 10:14 NS Operative time (min) 234 136 NS IV analgesia (days) 5.4 8.2 0.001 Morbidity (%) 18 50 0.02 Mortality 0 0 NS Inpatient rehabilitation 6 15 0.01 Hospitalization (days) 13.1 20.2 0.003 Teuch et al. Surg Endosc 2000
Costs: open vs. Laparoscopy *p<0.05 a = Total direct cost/case
Laparoscopy: Diverticulitis • There is good evidence (Level 2) that laparoscopy for diverticulitis results in earlier discharge
Laparoscopy: Diverticulitis • Despite longer operative time, the morbidity rate for the laparoscopic approach to diverticulitis in the most recent studies is equivalent or better than the open approach (Level 2 evidence)
Laparoscopy: Diverticulitis Conclusion • Elective laparoscopy for diverticular disease confers many advantages over the traditional approach • Based upon these data, laparoscopy is our preferred approach to the treatment of sigmoid diverticulitis
Practice Parameters for Sigmoid Diverticulitis The Standards Committee of The American Society of Colon and Rectal Surgeons The laparoscopic approach is appropriate in selected patients. Level of Evidence III, Grade of Recommendation A Laparoscopic colectomy may have advantages over open laparotomy, including less pain, smaller scar, and shorter recovery. There is no increase in early or late complications. Cost and outcome are comparable to open resection. Laparoscopic surgery is acceptable in the elderly and seems to be safe in selected patients with complicated disease Rafferty et al, DCR 2006