Download

1 / 46
460 likes | 538 Views
Explore the phases of diagnostic research from design to evaluation of diagnostic tests with real-life case studies and examples. Learn about the validity, reproducibility, and reliability of index tests using innovative methodologies. Join the Basic Residential Course at Palazzo Feltrinelli, Italy, to delve into the intricacies of diagnostic research.

E N D
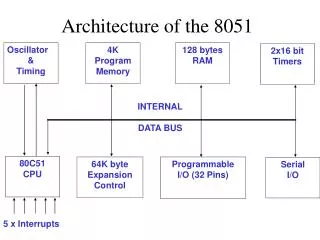
The architecture of diagnostic research Dario Conte, M.D. Gastroenterology and Endoscopy Unit Fondazione IRCCS “Cà Granda” Ospedale Maggiore Policlinico - Milano Università degli Studi di Milano Diagnosis - The pathway of a diagnostic test from bench to bedside Basic Residential Course April 4 – 8, 2017 - Palazzo Feltrinelli Gargnano - Lago di Garda - Italy
Phase IV Phase III 2d II a Phase II II b Phase I Phase 0
Phase IV Is the diagnostic test / therapeutic outcome in consecutive patient series studies in accordance with the results from randomized clinical trials? Phase III Do the tested patients fare better than comparable patients tested by a standard method or not tested? Phase IIb What is the proportion of false results in the two diagnostic strategies? Phase IIa Which of two tests is more accurate? Phase II Is the index test able to distinguish patients with and without the target disease among patients suspected of having the target disease? Phase I What is the range of the index test results in healthy people and the influence of sex, age, etc. Phase 0 What is the validity reliability and reproducibility of the index test (pre-clinical phase)
Phase 0 Validity The extent to which a test measures what it is intended to measure Transient elastography (TE): a new method for measuring the shear velocity in soft tissues Does TE provide a valid measure of liver stiffness? Elasticity Probe for Soft Tissues with 1-D TE Sandrin L IEEE Trans UltrasonFerroelectrFreq Control. 2002
Transientelastography − Reproducibility • 200 consecutive patients with chronic liver disease of different etiology, concurrently assessed by both TE and liver biopsy • 800 measurements performed Intra-observeragreement: 0.98 Intra-observeragreement: 0.98 Inter-observeragreement: 0.98 (95% CI: 0.977–0.987) Fraquelli et al. Gut 2007
Phase I - Example Aim: normal values definition Del Poggio et al. WJG 2009
Phase II – Preliminary questions Before the evaluation of the IT diagnostic accuracy, the phase II studies can address other preliminary questions
Phase II – Preliminary questions Discriminationbetweenhealthy and diseasedindividuals
Spectrum effects: evaluation of two very different populations Diagnostic Case Control Study Diagnostic Case Control Study Test threshold Healthy volunteers Test threshold % Healthy volunteers Very sick individuals Test parameter Test parameter
Study Design (cross-sectional) Case-control studies Cohort studies Clinically relevant cohort Consecutive patients with suspected target disease Reference Standard Disease + Disease – Case Control TEST Pos Neg TEST Reference Standard SPECTRUM VARIATION the sickest the healthiest SPECTRUM BIAS
Phase II – Preliminary questions Example Do test results in affected patients differ from those in healthy individuals? Are splachnicveins eco-doppler variablessignificantlydifferent in cirrhoticpatientsthan in healthycontrols ? 100 consecutive cirrhoticpatients vs 100 pair-matchedcontrols Eco-doppler signssignificantlydifferent Zoli et al. J UltrasoundMed 1985
Phase II – Preliminary questions Discriminationbetweendifferentdiseases or differentdisease stage
Phase II – Preliminary questions Example Noninvasive assessment of liver fibrosis by measurement of stiffness in patients with chronic hepatitis C 327 consecutive patients with HCV-related CLD: TE and LB Ziol et al. Hepatology 2005
Phase II - Preliminary questions • Discrimination between different diseases
Phase II – Preliminary questions Example Are the test results more likely to be abnormal in patients with disease different from or concurrent with the target disease than in patients with the target disease alone ? In 10 CHB patients and hepatitis exacerbations, the liver stiffness values paralleled those of ALT, increasing from 1.3- to 3-fold during ALT flare IT results are influenced by the presence of acute hepatitis with inflammation and necrosis ( concurrent disease) on chronic hepatitis with fibrosis (TD) Coco et al. J Viral Hepat 2007
Phase II - Preliminary questions Discrimination between different diseases
Phase II – Preliminary questions Example Decompensated chronic heart failure: increased liver stiffness measured by means of transient elastography 27 patients with heartfailurebut withoutsigns of liverdisease 21 controls, withoutheart and/or liverdisease underwent TE determinationat 0 time and atdischarge Sample size: Usual methods for comparison of proportions Colli et al. Radiology 2010
Phase II – Preliminary questions Example Intestinal lymphangectasia and reversible high liver stiffness Milazzo et al. Hepatology 2014
Phase II – Assessment of diagnostic accuracy Aim: to assess the diagnostic accuracy of the index test (IT) Diagnostic accuracy: measure of agreement between the IT and the RS in discriminating between diseased and non diseased participants
_ Study design Basic design of diagnostic accuracy studies: Prospective, blinded cross classification of test and reference standard in a clinical relevant setting TP Reference standard FP “Relevant” spectrum of patients IndexTEST FN Reference standard TN
Phase II - Example Diagnosis of cirrhosis by transient elastography (Fibroscan): a prospective study TE in 711 patients with CLD of different etiology (354 with liver biopsy) Foucher et al. Gut 2006
REFERENCE STANDARD = Liver biopsy Pos Neg INDEX TEST= TE Sensitivity TP / (TP+FN) Specificity TN / (TN+FP))
Diagnostic accuracy Foucher et al. Gut 2006
Spectrum effects: evaluation of representative populations Diagnostic Cohort Study Test threshold Patients without disease % Patients with disease Test parameter
Phase II a IT diagnostic accuracy and comparison of accuracies
Phase II a - Example • In the assessment of liverfibrosis an RCT compared the accuracy of twodifferentbiopsyneedles (Trucut vs Menghini) in the diagnosis of livercirrhosis: • 1.192 patientswererandomized to one of the twoneedles and a significantdifference in diagnosticaccuracywasfound Colombo et al. Gastroenterology 1988
Phase II b Proportion of false results of current diagnostic evaluation compared to that incorporating the IT (Safety or Benefit)
Phase II b - Example • Liverstiffnessmeasurement (LSM) is an accurate test for livercirrhosis • Ideal study: to estimate the cumulative incidence of FN patientsrandomizingpatients with suspectedcirrhosis to LSM or liverbiopsy • Patientsclassifiedascirrhoticsshouldundergoendoscopy • The comparison of the negative resultscouldidentify the safer procedure
Phase III Do the tested patients fare better than comparable patients tested by a standard method or not tested? Study design : RCT on diagnostic plus therapeutic strategies.
Eligibility criteria Studygroup suspected of having the target condition Randomise TE LB - - + + Treat Treat Do not treat Do not treat Outcome Outcome
Phase IV Benefits and harms of the IT-treatment strategy into the clinicalpractice • RCT • Large cohorts study • To assess in case of discordance between the IT and RS results what are the right results and • The proportion of patients with rare adverse events from the diagnostic test-therapeutic strategy
Phase IV – Example (A1) Noninvasive tests for fibrosis and liver stiffness predict 5-year outcomes of patients with chronic hepatitis C 1457 consecutive patients with chronic hepatitis C, in the same day, underwent: LSM, FibroTest, the AST/PTL ratio index FIB-4 and liver biopsy. Vergniol et al. Gastroenterology 2011
Phase IV – Example (A2) Vergniol et al. Gastroenterology 2011
Phase IV – Example (A3) Vergniol et al. Gastroenterology 2011
Phase IV – Example (B) Performances of LS and HVPG for the prediction of PH-related complications All patients Cirrhotics Robic et al. J Hepatol 2011
Phase IV – Example (C) Prognostic value of TE in the context of cirrhosis Cumulative risk for HCC in 866 HCV patients Masuzaki et al. Hepatology 2009
Acknowledgements (I) • Let me thank for their continuous support in planning this Course the following Colleagues and friends : • Giovanni Casazza, Agostino Colli, Gennaro D’Amico, Piergiorgio Duca, Mirella Fraquelli, Christian Gluud, DimitrinkaNikolova and Daniele Prati • All of us are deeply indebted to Sara Comparetti for the tremendous amount of work spent in organizing all the details of the Course itself and to Manuela Randazzo for the secretarial help
Acknowledgements (II) Moreover I would thank all of you for having attended this reading which is dedicated to Alessandro Liberati MD-PhD, an extraordinary man , a great scientist , a methodologist of international renown, a sower of culture , a doctor from the inexhaustible vitality and interest unlimited, a friend