Guillain-Barre Syndrome
410 likes | 1.26k Views
Guillain-Barre Syndrome. DR. INTEKHAB AHMAD 25 JAN 2010. Definition. It is an acute inflammatory demyelinating polyneuropathy leading to progressive muscle weakness & areflexia. Guillain Barre Syndrome. Commonest cause of rapid-onset flaccid paralysis since polio decline

Guillain-Barre Syndrome
E N D
Presentation Transcript
Guillain-Barre Syndrome DR. INTEKHAB AHMAD 25 JAN 2010
Definition It is an acute inflammatory demyelinating polyneuropathy leading to progressive muscle weakness & areflexia.
Guillain Barre Syndrome • Commonest cause of rapid-onset flaccid paralysis since polio decline • Occurs as an autoimmune response following a GI or respiratory infection • Potentially severely debilitating disorder affecting 1-3 per 100,000 • 10% die from associated complications • A further 10% suffer from long term neurological sequelae and physical dependence
History • Guillain, Barre and Strohl first described a disease affecting French soldiers ( motor weakness, areflexia and CSF abnormalities) in 1916 • Descriptions date back to 1859 when Landry described ascending paralysis
Aetiology • All ages affected with bimodal distribution towards young adults and the elderly • Slight male preponderance • Children less severely affected • Most commonly occurs within a month of GI or resp upset. • Commonest organism is campylobacter • Others inc EBV, CMV, HIV, herpes & mycoplasma
Have been reports of association with vaccines, surgery, epidurals, bone marrow and organ transplantation, SLE, lymphoma, sarcoidosis • Pregnancy and OCP confer some protection
Pathogenesis • Immunologically mediated nerve injury • Inflammatory cell infiltrates are seen in association with the demyelination, which is regarded as the primary pathological process • Precise mechanism of sensitisation not known • Antibodies formed against nonself antigens (inf agents,vacc) but misdirected to host nerve tissue (neural target- gangliosides) due to molecular mimicry leading to demyelination
Figure 1. Structural components of peripheral nerves. In the endoneurial compartment (En), a single Schwann cell envelops several unmyelinated axons, and another Schwann cell provides multiple wrappings of plasma membrane forming the myelin sheath of a myelinated axon. The portion of a myelinated axon myelinated by a single Schwann cell is called the internode, and internodes are separated by nodes of Ranvier. Schwann cells associated with both unmyelinated and myelinated axons are covered with a continuous basal lamina (BL). Capillaries (Cap) are present within the endoneurial compartment, and collagen fibers (Col) run primarily longitudinally between the axons. The axons, Schwann cells, collagen, and endoneurial fluid are bundled into a fascicle by the perineurium (Pe). The perineurium consists of several layers of flattened perineurial cells connected by tight junctions and covered internally and externally by a basal lamina. The layers of perineurial cells are separated by collagen fibers (Col) oriented obliquely. Several fascicles are bundled together by the epineurium (Ep) to form a nerve. The epineurium consists primarily of fibroblasts, collagen fibers (Col), and elastic fibers. The epineurium between fascicles is termed the interfascicular epineurium, and that encompassing all of the fascicles is termed the epifascicular epineurium. Arterioles (A) and veins are oriented primarily longitudinally within the epineurium.
Distributed throughout the nerve length but focused at nerve roots, spinal nerves and major plexuses • Macrophages actively strip myelin from bodies of schwann cells and axons • Underlying immune response is complex • Effectiveness of plasma exchange and IgG is thought to be blocking of demyelinating antibodies
VARIANTS • Several distinct clinical pictures described • Acute inflammatory demyelinating polyradiculopathy (AIDP) • Acute motor axonal neuropathy (AMAN) • Acute motor sensory axonal neuropathy (AMSAN) • Miller-Fisher syndrome ( ataxia, areflexia and opthalmoplegia ) which may be accompanied by limb weakness, ptosis and facial and bulbar palsy
Clinical presentation • Classical picture is that of ascending limb weakness with areflexia, although a purely sensory variant has been well documented • Features of GBS include • Progressive motor weakness, usually ascending from the legs • Areflexia • Facial palsy and bulbar weakness • Sensory symptoms—mainly subjective • Bladder/bowel—in severe cases
Severe pain esp girdle • Resp muscle weakness • Autonomic dysfunction( over or underactivity of the SNS or PSNS)
Features required for diagnosisdefined by national institute of neurological and communicative diseases and strokes • Progressive muscle weakness of more than one limb • Areflexia or marked hyporeflexia • CSF cell counts of no more than 10 • Features highly suggestive • Features required to rule out other diagnosis
Doughtful diagnosis • Definite sensory level • Marked, persistent asymmetry of motor weakness • Severe & persistent bladder/bowel dysfunction • CSF cell count > 50
Monitoring • Cardiac • Blood pressure • Vital capacity measured three times a day • Bulbar function monitored to prevent aspiration
Investigations • In over 90% patients CSF protein is raised ( >0.4g/l) within a week of onset of symptoms • Level does not correlate with clinical findings • Nerve conduction studies demonstrate reduced conduction velocity • Liver and renal function may be impaired • Antiganglioside antibody should be searched for
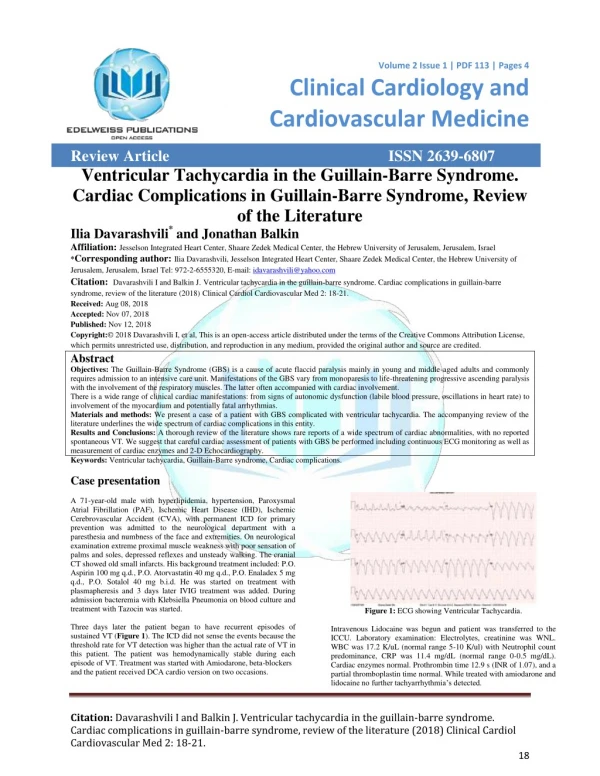
SIADH may occur in association with GBS • Stool cultures for campylobacter • Ecg’s for QT, T and ST abnormalities • Head CT to exclude raised ICP and other pathology prior to LP
Treatment • Major challenge • Outcome excellent if complications treated or avoided • Prevented by meticulous attention to detail
Specific treatment-disease modifying modalities • Plasma exchange • Immunoglobin • Both should be used when patient non-ambulatory or resp decompensation occurs • Both have been examined in RCT and no difference in efficacy demonstrated between them
Plasma exchange • 2 RCT showed reduction in ventilation and reduced time to motor recovery • Mortality was not altered • Most effective within 7 days of onset • 3-5 exchanges of 1-2 plasma volumes each over 1-2 weeks • Ffp more complications than albumin • CI include CVS instability, sepsis and haemostatic problems • Side effects are hypotension, hypocalcaemia,coagulation abnormalities and sepsis
IV Immunoglobin • 0.4mg/kg daily for 5-6 days • Easier administration • Fewer side effects • Commence tx within 2 weeks of onset of symptoms • CI include IgA deficiency(anaphylaxis) • Renal function may deteriorate • Severe congestive cardiac failure major contraindication • RCT has suggested as effective as plasma exchange
Steroids • No place in the treatment of GBS • RCT have shown no advantage
CSF filtration • Few case reports • When plasmapheresis and IgG have failed • Logistics difficult!
Supportive care • Respiratory, • 25% require ventilated • Physio and VC monitoring in the spont breathing. If less than 15ml/kg or rising pCO2, mechanical ventilation likely • Monitoring of bulbar function for prevention of aspiration • Non-invasive ventilation often not useful as does not eliminate the problem of not being able to clear secretions due to poor cough • Early tracheostomy should be considered
Supportive care • Cardiovascular • Full invasive monitoring • Care with induction of anaesthesia as leads to hypotension and arrhythmias • Care with suxamethonium may lead to arrhythmias • Instability may be worsened by other drugs • Autonomic instability common
Supportive care • Nutrition, fluid and electrolytes • Paralytic ileus common • Tpn may be required • Energy and fluid requirements are reduced in these patients • Physiotherapy • DVT prophylaxis • Sepsis survellience • Psychological care • analgesia
Prognosis • Death in up to 25% of those who require ICU has been reported often from autonomic abnormalities • Approx 16% patients suffer permanent disability • Those who require ventilation, improve after more than 3 weeks, not improved within 1 month have greater risk of poorer outcome • Gradual improvement may occur over 18months -2years • Recurrence n 2-5% cases