Download
1 / 32
630 likes | 1.93k Views
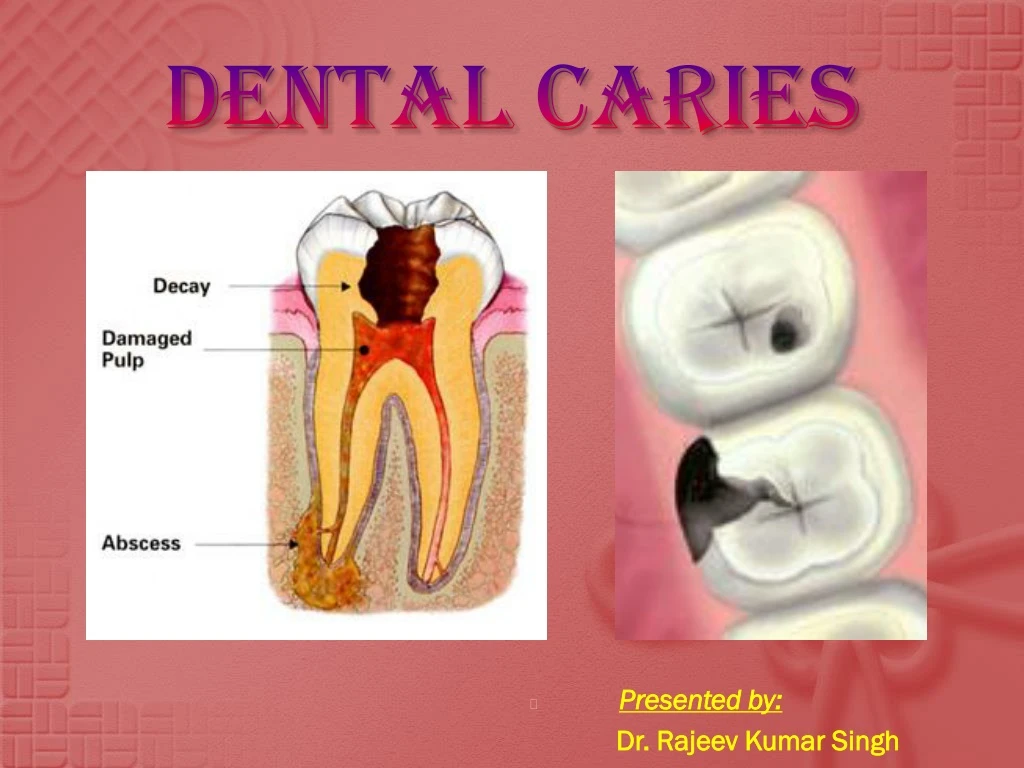
DENTAL CARIES. Presented by: Dr. Rajeev Kumar Singh. Historical background. Archaeological evidence shows that tooth decay is an ancient disease dating far into prehistory Tooth worms were considered to be the cause.

E N D
DENTAL CARIES • Presented by: Dr. Rajeev Kumar Singh
Historical background Archaeological evidence shows that tooth decay is an ancient disease dating far into prehistory Tooth worms were considered to be the cause. Many believed that the tooth worm bore a hole through the tooth, hiding beneath the surface. Historical evidence suggest that Chinese used acupuncture around 2700 BC to treat pain associated with tooth decay.
Pierre Fauchard, known as the father of modern dentistry, was one of the first to reject the idea that worms caused tooth decay and noted that sugar was detrimental to the teeth and gingiva In the 1890s, W.D. Miller conducted a series of studies that led him to propose an explanation for dental caries that was influential for current theories.
The dental drill dates back 9,000 years ago The tooth worm as Hell’s demon: a battle with the “tooth worm”
Definition Dental caries is a microbial disease which causes dissolution of inorganic and destruction of organic component of the tooth leading to cavitation. It is a dynamic process with episodes of demineralization and remineralization. Dental caries is a preventable disease.
Etiology Dental caries an infectious disease, the initiation & progression of which is influenced by multiple factors. W. D. Miller proposed the chemopasitic theory (acidogenic theory) in 1890. The main features of this theory are:- The carious process require a host (tooth in the oral environment), a dietary substrate and acidogenic bacteria. The presence of fermentable carbohydrate serves as nutrient for bacteria. These bacteria produce organic acids that can demineralize the tooth.
Two groups of bacteria are primarily responsible for initiating of dental caries: Streptococcus mutans and Lactobacilli. These bacteria in the presence of fermentable carbohydrate (such as sucrose, fructose & glucose) produce organic acids(lactic acid) which leads to dissolution of enamel. These bacteria also produce proteolytic enzymes which are responsible for breakdown of organic macromolecules after demineralization leading to cavitation.
Stephan curve Apart from the three primary factors, time also plays an important role in initiation of caries. Robert Stephan plot a curve of plaque pH against time known as Stephan curve. Plaque pH falls from an average of 6.8 to 5 within 2-3 minutes of eating sugar or rinsing with a sugar solution & takes about 40 minutes to return to its original value. The demineralization of enamel occurs below pH 5.5(Critical pH)
Caries balance The development of caries may be considered as a continuous dynamic process involving repeating episodes of demineralization by organic acids and subsequent demineralization by salivary components or therapeutic agents but in which the overall oral environment is imbalanced towards demineralization. Saliva plays an important role in remineralization of incipient caries. Protective factors which include salivary calcium, phosphate and proteins, salivary flow, and fluoride in saliva can balance, prevent or reverse dental caries.
Pathogenesis Enamel caries Enamel is destructed by a chemical process brought on by the acidic environment produced by bacteria who consume the sugar for their own energy & produce lactic acid. This process demineralizes the enamel crystals over time until the bacteria physically penetrate the dentin. Enamel rods run perpendicular from the surface of the tooth to the dentin. Different triangular patterns between pit and fissure and smooth-surface caries develop in the enamel because the caries follows the direction of enamel rods & orientation of enamel rods are different in the two areas of the tooth.
As the enamel loses minerals , and dental caries progress, they develop several distinct zones, visible under a light microscope. From the deepest layer of the enamel to the enamel surface, the following identified areas are present:- Translucent zone Dark zones Body of the lesion Surface zone.
The translucent zone is the first visible sign of caries and coincides with a 1-2% loss of minerals. A slight remineralization of enamel occurs in the dark zone, which serves as an example of how the development of dental caries is an active process with alternating changes. The area of greatest demineralization and destruction is in the body of the lesion itself. The surface zone remains relatively mineralized and is present until the loss of tooth structure results in a cavitation.
Dentinal caries Unlike enamel, the dentin reacts to the progression of dental caries. After tooth formation the ameloblasts are destroyed, once enamel formation is complete and cannot later regenerate enamel after its destruction. On the other hand, dentin is produced continuously throughout life by odontoblasts, which reside at the border between the pulp and dentin. A carious stimulus can trigger a biologic response by odontoblasts. These defense mechanisms include the formation of sclerotic and tertiary dentin.
In dentin from the deepest layer to the enamel, the distinct areas affected by caries are the:- Translucent zone Zone of bacterial penetration Zone of destruction The translucent zone represents the advancing front of the carious process and is where the initial demineralization begins. The zones of bacterial penetration and destruction are the locations of invading bacteria and ultimately the decomposition of dentin.
Rampant caries Suddenly appearing, widespread, rapidly burrowing type of caries, resulting in early involvement of the pulp and affecting those teeth usually regarded immune to dental decay. Specific Features :- Sudden, rapid and almost uncontrollable destruction of teeth. Surface considered immune to decay are involved. Thus, mandibular incisors are affected. A caries increment of 10 or more new carious lesions over a period of about a year.
Most observed in primary dentition of young children & permanent dentition of teenagers, 11-19 years Types :- Nursing Bottle caries Adolescent caries Causes :- Xerostomia Drug induced dry mouth Large sugar intake Emotional disturbances Radiation therapy
Nursing bottle caries According to AAPD, early childhood caries is characterized by the presence of one or more decayed, missing(due to caries) or filled tooth surfaces in any primary tooth in a child 71 months of age or younger. Also known as: Baby Bottle Tooth Decay (BBTD) Infant caries Bottle mouth syndrome Early Childhood Caries (ECC)
Etiology :- Nursing bottle feeding holding milk or sugar containing beverages before & during sleep Prolonged bottle or breast feeding Pacifiers dipped in honey / other sweeteners.
Classification Moderate Mild Severe
Clinical features Caries follow the particular teeth eruption order pattern Upper primary incisors affected first followed by upper first primary molars Lower first primary molars Mandibular canines sometimes Mandibular incisors are usually unaffected.
Complications Pain Tooth abscess Tooth loss Broken teeth Chewing problems Serious infections
Management Management of pain at first visit Pain is a common complication of ECC Excavation & appropriate dressing of teeth with ZOE or dilute formocresol will usually help to temporarily manage pain and localized infection. Antibiotics should be prescribed in acute soft tissue swelling or signs of systemic involvement Child should be referred to specialist for urgent management in case of increasing facial swelling or serious systemic involvement
Comprehensive treatment All lesions should be excavated and restored. X-rays are advised to assess the condition of the succedaneous teeth. Treatment depends on how far the disease has progressed Very early detection-topical fluoride application and diet modification. Obvious decay – stainless steel crowns or veneered crowns. Severe decay – Pulp therapy followed by crown placement. In case of unrestorable teeth, extractions can be done followed by space maintenance.
Prevention Role of Parents Clean your child's teeth daily. Never allow your child to fall asleep with a bottle filled with juice, milk or formula. Start bottle weaving by at least a year. Give your child plain water for thirst. Make sure your child gets the fluoride needed to prevent decay. Have regular dental visits for your child beginning when their first tooth erupts.
Role of Dentist To create awareness and alert prospective parents and new parents about the conditions and its cause. Sealing of all caries free pits and fissures. Professional fluoride programme. Supervised home care should be taught. Systemic fluoride programme if there is suboptimal fluoride concentration in drinking water.