Download
1 / 1
20 likes | 263 Views
Carnitine-Acylcarnitine Translocase Deficiency and Pregnancy: A Case Report Harding L 1 , Crane J 1 , Turner L 2 , Brown K 1 . Department of Obstetrics and Gynecology 1 and Department of Genetics 2 Memorial University, St. John’s, Newfoundland. Results. Abstract

E N D
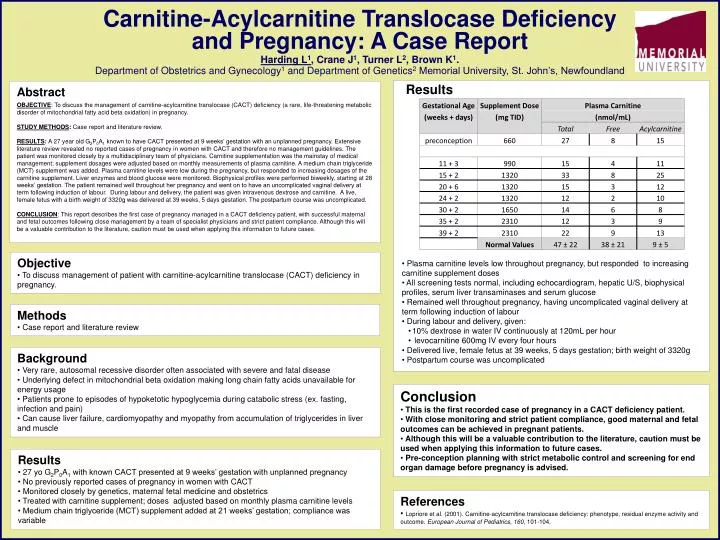
Carnitine-Acylcarnitine Translocase Deficiency and Pregnancy: A Case Report Harding L1, Crane J1, Turner L2, Brown K1. Department of Obstetrics and Gynecology1 and Department of Genetics2 Memorial University, St. John’s, Newfoundland Results Abstract OBJECTIVE: To discuss the management of carnitine-acylcarnitine translocase (CACT) deficiency (a rare, life-threatening metabolic disorder of mitochondrial fatty acid beta oxidation) in pregnancy. STUDY METHODS: Case report and literature review. RESULTS: A 27 year old G2P0A1 known to have CACT presented at 9 weeks’ gestation with an unplanned pregnancy. Extensive literature review revealed no reported cases of pregnancy in women with CACT and therefore no management guidelines. The patient was monitored closely by a multidisciplinary team of physicians. Carnitine supplementation was the mainstay of medical management; supplement dosages were adjusted based on monthly measurements of plasma carnitine. A medium chain triglyceride (MCT) supplement was added. Plasma carnitine levels were low during the pregnancy, but responded to increasing dosages of the carnitine supplement. Liver enzymes and blood glucose were monitored. Biophysical profiles were performed biweekly, starting at 28 weeks’ gestation. The patient remained well throughout her pregnancy and went on to have an uncomplicated vaginal delivery at term following induction of labour. During labour and delivery, the patient was given intravenous dextrose and carnitine. A live, female fetus with a birth weight of 3320g was delivered at 39 weeks, 5 days gestation. The postpartum course was uncomplicated. CONCLUSION: This report describes the first case of pregnancy managed in a CACT deficiency patient, with successful maternal and fetal outcomes following close management by a team of specialist physicians and strict patient compliance. Although this will be a valuable contribution to the literature, caution must be used when applying this information to future cases. • Plasma carnitine levels low throughout pregnancy, but responded to increasing carnitine supplement doses • All screening tests normal, including echocardiogram, hepatic U/S, biophysical profiles, serum liver transaminases and serum glucose • Remained well throughout pregnancy, having uncomplicated vaginal delivery at term following induction of labour • During labour and delivery, given: • 10% dextrose in water IV continuously at 120mL per hour • levocarnitine 600mg IV every four hours • Delivered live, female fetus at 39 weeks, 5 days gestation; birth weight of 3320g • Postpartum course was uncomplicated • Objective • To discuss management of patient with carnitine-acylcarnitine translocase (CACT) deficiency in pregnancy. • Methods • Case report and literature review • Background • Very rare, autosomal recessive disorder often associated with severe and fatal disease • Underlying defect in mitochondrial beta oxidation making long chain fatty acids unavailable for energy usage • Patients prone to episodes of hypoketotic hypoglycemia during catabolic stress (ex. fasting, infection and pain) • Can cause liver failure, cardiomyopathy and myopathy from accumulation of triglycerides in liver and muscle • Conclusion • This is the first recorded case of pregnancy in a CACT deficiency patient. • With close monitoring and strict patient compliance, good maternal and fetal outcomes can be achieved in pregnant patients. • Although this will be a valuable contribution to the literature, caution must be used when applying this information to future cases. • Pre-conception planning with strict metabolic control and screening for end organ damage before pregnancy is advised. • Results • 27 yo G2P0A1 with known CACT presented at 9 weeks’ gestation with unplanned pregnancy • No previously reported cases of pregnancy in women with CACT • Monitored closely by genetics, maternal fetal medicine and obstetrics • Treated with carnitine supplement; doses adjusted based on monthly plasma carnitine levels • Medium chain triglyceride (MCT) supplement added at 21 weeks’ gestation; compliance was variable • References • Lopriore et al. (2001). Carnitine-acylcarnitine translocase deficiency: phenotype, residual enzyme activity and outcome. European Journal of Pediatrics, 160, 101-104.