Download
1 / 11
110 likes | 265 Views
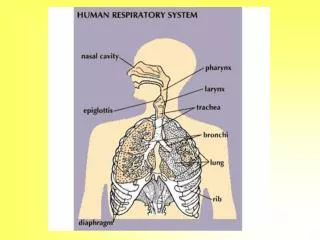
How do we breath?. INHALATION: The diaphragm and intercostal muscles contract causing the diaphragm to move down slightly. This enlarges the thoracic cavity, and the ribs rise up and out. This lowers inside pressure, causing outside air to enter lungs EXHALATION:

E N D
How do we breath? INHALATION: The diaphragm and intercostal muscles contract causing the diaphragm to move down slightly. This enlarges the thoracic cavity, and the ribs rise up and out. This lowers inside pressure, causing outside air to enter lungs EXHALATION: The diaphragm and intercostal muscles relax, causing pressure to increase. The thorax decreases in size, and the ribs and muscles assume a normal resting position. Air rushes out of lungs.
Man, I’m sensing lots of C02…the lungs better suck in some 0’s! The level of C02 bathing the brain stem is what stimulates a healthy person to breathe.
Hypoxia - What do you see (S/S): Body’s tissues and cells do not have enough oxygen • Change in mental status - irritability, restlessness, disorientation, combativeness • Visible “work of breathing” - nasal flaring, tracheal tugging, sternal & costal retractions, belly breathing, tripod position • Signs of Inadequate Respirations - dyspnea; incomplete sentences; air hunger; gasping - inadequate respiratory rate and tidal volume - abnormal respiration sounds (eg wheezing, rales, gurgling) • Signs of Shock
What is adequate Respiration? Normal Respiration Rate Adult – 12 to 20 breaths/min Children – 18 to 34 breaths/min Infants – 30 to 60 breaths/min BUT ---- Respiration Rate alone is NOT the criteriaLook for combination of respiration rate and tidal volume (eg rapid & shallow = BAD)
What do you do : The patient is failing the ABCs • Locate/treat cause, if possible • Give immediate O2 • Support respiration • Monitor vitals every 5 mins • Emergency evacuation
Causes of Hypoxia: CHRONIC CONDITIONS • COPD = slow process of lung disintegration; usually seen as emphysema and/or bronchitis • CYSTIC FIBROSIS – inherited mucus condition ACUTE CONDITIONS • ANAPHYLACTIC REACTION – closing air passages • ASTHMA – chronic condition with acute spasms UPPER AND LOWER AIRWAY INFECTIONS • Pneumonia, Croup, Epiglottitis, Bronchitis
Causes of Hypoxia: TRAUMA • BLUNT OR PENETRATING CHEST TRAUMA OTHER • PULMONARY EDEMA- fluid in lungs due to heart muscle dysfunction, smoke or toxins, • PULMONARY EMBOLISM – blockage of pulmonary arteries; sudden onset of pain • PULMONARY EFFUSION = fluid outside lungs, due to infection, CHF, cancer
Agonal Respirations A patient may appear to be breathing even after the heart has stopped beating. Cheyne-Stokes Respirations Irregular breathing followed by period of apnea; associated with stroke and serious head injuries
Key Items to Remember • Monitor the Airway… Could close at any time leading to unconsciousness • Transport – Position of Comfort, often sitting upright
When to use O2 1. any unconscious patient2. any patient with respiratory distress – trauma or medical3. any patient with altered mental status4. any patient with signs of shock5. any patient with severe pain - fractures, dislocations, etc