Download
1 / 13
130 likes | 203 Views
Learn about ACCORD trial's design, goal to reduce CVD events by targeting hyperglycemia, dyslipidemia, and high blood pressure. Discover results, eligibility criteria, outcomes, and treatment strategies.

E N D
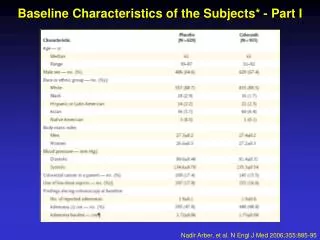
ACCORD Design and Baseline Characteristics Presented at the American Diabetes Association 68th Scientific Sessions on June 10, 2008.
ACCORD Trial Overall Goal To determine whether CVD event rates can be reduced in people with diabetes by intensively targeting three important CVD risk factors: hyperglycemia, dyslipidemia, and high blood pressure. Three trials in one research program Double 2 by 2 factorial design
Glycemia Trial Research Question • In middle aged/older people with type 2 DM at high risk for a CVD event, does a therapeutic strategy that targets an A1C < 6.0% reduce CVD event rates more than a strategy that targets an A1C between 7.0% & 7.9% (with the expectation of achieving a median level of 7.5%)?
Observational studies supportive Each 1% higher A1C associated with 18% greater risk of CVD1 CVD-glucose relationship extends into the normal range Clinical trials inconclusive2 Glycemia Trial Rationale 1. Selvin E, et al. Ann Intern Med. 2004;141:421-431. 2. Goff DC Jr, et al. Am J Cardiol. 2007;99[suppl]:4i-20i.
ACCORD Design • Multi-center, randomized, controlled, double 2x2 factorial • Glycemia and BP Trials Open Label with Blinded Endpoint Assessment • Lipid Trial placebo controlled • Glycemia Trial • 89% power to detect a 15% difference in major CVD events between treatment groups. • Assumed at least 1% difference in A1C needed • Goal A1C difference 1.5% • Expected primary event rate about 3% per year • Sample size goal 10,000 • 77 clinics in US and Canada
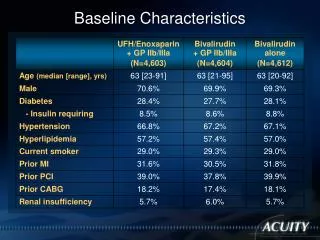
Double 2 X 2 Factorial Design BP Lipid Intensive (SBP<120) Standard (SBP<140) Statin + Masked Study Drug Statin + Masked Study Drug Intensive Glycemia (A1C<6%) 1178 1193 1383 1374 5128* Standard Glycemia (A1C 7-7.9%) 1184 1178 1370 1391 5123* 2371* 2753* 2765* 10,251 2362* *Primary analyses compare the marginals for main effects
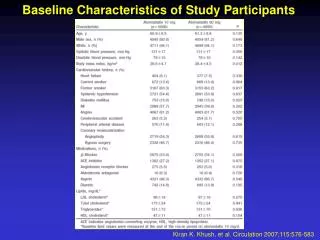
Participant Eligibility • Stable Type 2 Diabetes for 3+ months • A1C >7.5% AND <9% (more meds)OR <11% (fewer meds) • Age 40-79 + previous CVD events OR • Age 55-79 with: • anatomical ASCVD, albuminuria, LVH OR • > 2 CVD risk factors (dyslipidemia, hypertension, smoking, obesity) • BMI < 45; Cr <1.5 (133 uM) • No frequent/recent serious hypoglycemia • Able/willing to take insulin, do glucose monitoring • Eligible for BP or Lipid Trial
ACCORD Outcomes • Primary: • First occurrence of nonfatal MI OR Nonfatal Stroke OR CV Death • Secondary/Other: • Each component of 10 • Expanded CVD: 10 + Revasc & HF Hosp • Total mortality • Microvascular (nephropathy, neuropathy, eye) • Eye photo substudy (N = 3537) • HRQL (N = 2053); Cost (N = 4311) • MIND: cognition, brain volume (MRI) • Falls/Fractures/BMD
Treatment Strategies • Compared with the standard group, the intensive group had: • Lower A1C goal (< 6% vs. 7 - 7.9%) • More visits (q 1-2 mo + at least 1 interim call vs. q 4 mo) • Point of care A1C • Greater use of multiple medications • Greater use of insulin
ACCORD Trial Design Summary • Large complex research program • Multi-center, randomized, controlled factorial trials of 3 approaches to reduce CVD in T2DM • Glycemia Trial Open Label with Blinded Endpoint Assessment • Interventions designed to produce 1-1.5% difference in A1C • Goals: A1C < 6% vs 7 – 7.9% • Primary endpoint: major CVD events • Participants: diverse group of middle-aged and older adults with established T2DM with or at high risk for CVD • High use of evidence-based background therapies: ASA, ACE-I, BB, Statins • Results should be interpreted in context of population studied and other therapies received.