Download
1 / 1
10 likes | 201 Views
Ocular Complications of Smallpox Vaccination Elizabeth Clair, OMS III, Bryant Self, OMS IV, Kade Hardy, OMS III William Carey University College of Osteopathic Medicine (WCUCOM). SMALLPOX. CASE. LITERATURE REVIEW. The World Health Assembly declared smallpox eradicated worldwide in 1980.

E N D
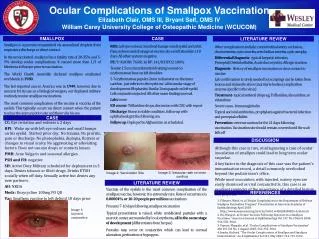
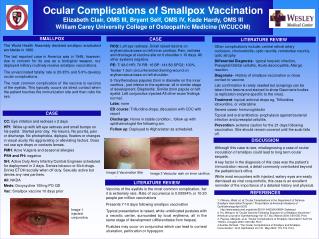
Ocular Complications of Smallpox Vaccination Elizabeth Clair, OMS III, Bryant Self, OMS IV, Kade Hardy, OMS III William Carey University College of Osteopathic Medicine (WCUCOM) SMALLPOX CASE LITERATURE REVIEW The World Health Assembly declared smallpox eradicated worldwide in 1980. The last reported case in America was in 1949, however, due to concern for its use as a biological weapon, our deployed military routinely receive smallpox vaccinations. The unvaccinated fatality rate is 20-35% and 5-9% develop ocular complications. The most common complication of the vaccine is vaccinia of the eyelids. This typically occurs via direct contact when the patient touches the immunization site and then rubs his eye. ROS: Left eye redness. Small raised lesions on erythematous base on left inner canthus. Pain, redness and drainage at vaccine site on lt shoulder x 10 days. All other systems negative. PE: T: 98.0 HR: 76 RR: 16 BP: 141/83 SPO2: 100% Tender 1.5cm circumferential draining wound on erythematous base on left shoulder. 5-7erythematous papules 2mm in diameter on the inner canthus , just inferior to the eyebrow- all in similar stage of development. Blepharitis. Similar 2mm papule on left eyelid. Left conjunctiva injected.All other exam findings normal. Labs: none ED course: Trifluridine drops, discussion with CDC with report Discharge: Home in stable condition , follow up with ophthalmologist the following am. Follow up: Deployed to Afghanistan as scheduled. Other complications include: central retinal artery occlusion, chorioretinitis, optic neuritis, retrobulbar neuritis, optic atrophy Differential Diagnosis- typical herpetic infection, Preseptal/Orbital cellulitis, Acute dacrocystitis, Allergic reaction Diagonsis- History of smallpox vaccination or close contact to vaccine Lab confirmation is rarely needed but scrapings can be taken from lesions and stained to show Gaurnierie bodies (a replication enzyme specific to the virus). Treatment- topical antiviral drops eg, Trifluridine, idoxuridine, or vidarabine Severe cases- Immunoglobulin Topical and oral antibiotics- prophylaxis against bacterial infection and preseptal cellulitis. Prevention- extreme caution for the 21 days following vaccination. Site should remain covered until the scab falls off. CASE CC: Eye irritation and redness x 2 days HPI: Woke up with left eye redness and small bumps on his eyelid. Started prior day. No trauma. No pruritis, pain or discharge. No photophobia, diplopia, floaters or changes in visual acuity. No aggravating or alleviating factors. Does not use eye drops or contacts lenses. PMH: Acne Vulgaris and seasonal allergies PSH and FH: negative SH: Active Duty Army Infantry/Combat Engineer scheduled for deployment in 3 days. Denies tobacco or illicit drugs. Drinks ETOH socially when off duty. Sexually active but denies any new partners. All: NKDA Meds: Doxycycline 100mg PO QD Vac: Smallpox vaccine 10 days prior . DISCUSSION Although this case is rare, misdiagnosing a case of ocular inoculation of smallpox could lead to long term ocular sequela. A key factor in the diagnosis of this case was the patient’s immunization record, a detail commonly overlooked beyond the pediatrician’s office. While most encounters with injected, watery eyes are easily dismissed as viral conjunctivitis, this case is an excellent reminder of the importance of a detailed history and physical. Image 2 Vaccination Site Image 3 Vesicular rash on inner canthus . LITERATURE REVIEW Vaccinia of the eyelids is the most common complication, iter it is extremely rare. Rate of occurrence is 0.00004% or 10-20 people per million vaccinations Presents 7-10 days following smallpox vaccination Typical presentation is raised, white umbilicated pustules with a necrotic center, surrounded by local erythema, all in the same stage of development (differentiates from herpes) Pustules may occur on conjunctiva which can lead to corneal ulceration, perforation or hypopyon. REFERENCES 1. Fillmore, Ward, et. al.“Ocular Complications in the Department of Defense Smallpox Vaccination Program.” Presentation at American Academy of Ophthalmology April 2003 http://www.aaojournal.org/article/S0161-6420(04)00824-3/abstract 2. Hu, Wang et. al.“Ocular Vaccinia Following Exposure to a Smallpox Vaccinnee.” American Journal of Ophthalmology Vol 137, No.3 March 2004: 554-556. Print. 3. Pepose, Margolis, et.al. “Ocular Complications of Smallpox Vaccination” AJO Vol 136 No. 2 August 2003: 343-352. Print. 4.Semba, Richard. “The Ocular Complications of Smallpox and Smallpox Immunization.” Arch Ophthalmol Vol 121, May 2003: 715-719. Print. Image 1 injected conjunctiva