Download
1 / 37
370 likes | 490 Views
This overview highlights the critical roles of thyroid hormones (T3 and T4) in regulating metabolism, growth, and development. Hypertension, mood alterations, and changes in weight may indicate thyroid dysfunction. Pediatric topics include congenital hypothyroidism and the significance of early diagnosis and treatment to prevent developmental issues. Additionally, this summary addresses autoimmune disorders like Hashimoto’s and the clinical implications of hyperthyroidism. Proper nursing interventions and lifelong treatment recommendations are discussed to ensure patient well-being.

E N D
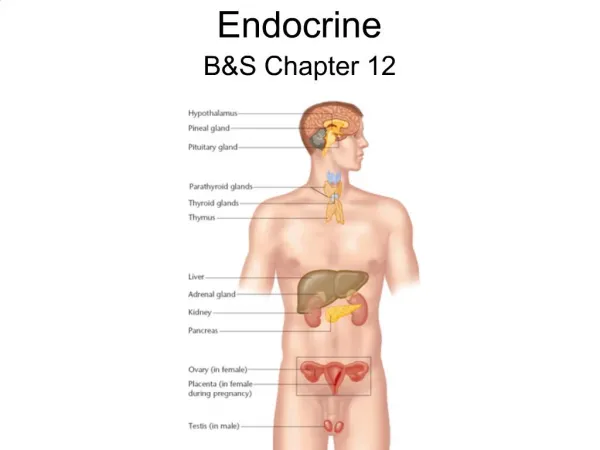
Endocrine Elisa A. Mancuso RNC-NIC, MS, FNS Professor of Nursing
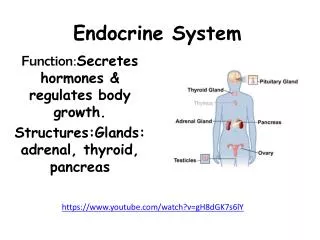
Hormones Regulate growth & activity of cells Interact with receptors of “target tissues” Regulate metabolism & stress response Maintain fluid & electrolyte balance Sexual reproduction Feedback mechanism ↑ Blood Level = ↓ Gland Secretion ↓ Blood Level = ↑ Gland secretion
Thyroid Gland • Takes up I & changes I to react with tyrosine • I + tyrosine → Thyroid hormones T4 + T3 • TSH secrets T4 & T3 • Dependent on blood levels • ↑ T4 or T3 = ↓ TSH • ↓ T4 or T3 = ↑ TSH
Thyroid Hormones Thyroxin- T4 • Maintains metabolism in steady state • Temp Cardiac GI Neuro • Cellular metabolic activity → Rate of O2 use • Stimulates growth and development • Protein synthesis & Tissue Differentiation • Essential for brain development in first 2 years Triidothyronine- T3 • Rapid & Intermediate metabolic actions Thyrocalcitonin • Maintain serum Ca++ & PO4 levels • ↑↑ Ca++ in serum →Calcitonin is released • ↓↓ Ca++ serum and promote Ca+ bone deposit
Hypothyroidism Most common pediatric endocrine disorder • Failure of Thyroid gland development (aplasia) • ↓↓ T3 and T4 • Initially provides enough T3 & T4 for 1st year. • Then unable to meet rapid body growth needs. • Anti-thyroid drugs or I deficiency during pregnancy • PKU-Phenylketonuria. • Genetic defect in synthesis of thyroxin. • Gunthrie Test (PKU) performed at 48 hours of life. • Unable to convert phenylalanine (amino acid) to tyrosine.
Congenital Hypothyroidism Cretinism- Infancy • Girls 3x more common • If not tested and untreated displays signs and symptoms in 3-6 weeks • Early DX best prognosis • Tx before 3 months and baby will grow and develop normally. • No treatment will lead to mental • retardation
Clinical Signs “Very Good Baby” • Lethargic & “sleeps well” • ↓ BMR ↑ weight, cold & mottled • Anorexia & Poor feeding • Hypotonia • Constipation • Hoarse cry • Dry Skin
Facial Features • Broad nose • Wide fontanels and sutures • Broad, flat nose • Protruding tongue • Short thick neck Disproportionate Body • Short arms & legs
Acquired HypothyroidismJuvenile • Lymphocytic thyroiditis- “Hashimoto’s” • Autoimmune Disease • Auto-antibodies bind to TSH receptor sites on thyroid gland • ↓ levels of T3 T4. • Atrophy of thyroid gland • Cause of antibody production unknown • Associated with goiter
Sign and Symptoms • ↓↓ Growth • Edema of face, eyes and hands • ↓ Decreased BMR • Increased weight gain • ↓ V/S = ↓ Temp, ↓ HR and ↓ BP • Lethargy • ↑ sensitivity to cold • Forgetfulness • ↓ Decreased mental alertness
Myxedema • Dry thicken skin • Fat accumulation • subcutaneous tissue • Brittle hair • coarse and sparse Diagnosis • Thyroid scan • TSH Radioimmunoassay • ↑TSH with ↓T3 and ↓ T4
Therapy Synthroid (l-thyroxine) 5-10 PO ug/kg/day • Individualized to pt’s TSH level • Initially low dose • Gradually ↑ (over 4-8 weeks) • Allow body time to adjust to changes • ↑ BMR & ↑ V/S • Monitor V/S, HR, Temp & BP! • Lifelong therapy • √ T3 & T4 q 6 months
Nursing Interventions • Activity • Accept pt’s lethargy • Need ↑ time to do ADLs • Skin care • Oils, lotions • Frequent position changes • Prevent chilling • Encourage layering of clothes • Diet • ↑Fiber ↑Protein ↑Vit D = ↑ Bone Growth • ↓ Cals ↓ Fats ↓ Fluids = ↓ Edema
Synthroid Toxicity Overdose of Medication • ↑Irritable & Nervousness • ↑ BMR & ↑ Temp ↑ HR ↑ BP • Wide pulse pressure • Diaphoresis, tremors, V & diarrhea • Therapy • √ serum T3 T4 • Hold med or ↓dose
Hyperthyroidism Neonatal hyperthyroidism • Maternal Grave’s disease • Thyroid Stimulating immunoglobulins (TSI), autoantibodies passed through the placenta to fetus. • TSI binds to TSH receptors = excess thyroid hormone production • Excessive maternal I exposure • Neonatal thyroid hypertrophy to uptake • excess I
Neonatal Graves Disease • Irritability • Tachycardia • Hypertension • Voracious appetite with FTT (↓ Weight) • Flushing • Prominent eyes • Goiter • Tracheal compression • ↑ Respiratory distress → asphyxia
Grave’s Disease Autoimmune condition • Thyroid stimulating immunoglobulin rxn = ↑ T3 T4 • Hyperplasia of thyroid gland • Develops gradually over 6 -12 months • Suppression of TSH = No Feedback mechanism • Peak incidence is 11 and 15 years • Girls 5 times > boys • + Family history of thyroid disease
Signs and Symptoms • Goiter • Exopthalmos • ↑↑ risk corneal abrasion • ↑↑ Appetite & ↓↓ weight • (-) N balance • ↑↑ VS @ rest • HR> 160 Palpitations • ↑ BP → CHF • ↑ Temp = Heat intolerance • Peripheral vasodilation • Flushed skin • ↓↓ Attention span • Emotional liability & cry easily
Medications Propylthiouracil (PTU) 50 – 100mg/day ÷ bid • Interferes with I conversion to thyroxine • Prevents T3 and T4 synthesis • Takes 3 - 4 weeks, No effect on available T3 T4 • Side Effects • Skin rash-urticaria, • Agranulocytosis- S/S of infection = STOP med! • Monitor for overdose • ↓ VS↑ Lethargy Sleepiness Methimazole (Tapazole) 0.2mg/kg q12H • Blocks formation of new T3 and T4. • Available T3 and T4 must be used up
Medications Potassium Iodine SSKI (Lugol’s solution) • ↓ pituitary TSH = ↓ Thyroxin ↓ T3 T4 • ↓ glands vascularity • used a surgery ↓bleeding • Side Effects • Swelling of salivary glands • Metallic taste, burning of mouth & throat. • Sore teeth & gums, skin rash • √ serum K+
Surgery Sub Total Thyroidectomy • Removes majority of gland 5/6 (leave isthmus. • Gradually takes over body’s needs • Hormone replacement initially • Then gradually taper off Post-op complications • Hemorrhage • √ blood behind neck ↑VS • Respiratory distress- • Laryngeal edema √ stridor (trach at bedside) • Dysphasia • Laryngeal nerve damage √ speech
Thyroid Storm Life Threatening Crisis • Acute infection or Post-op • Manipulation of thyroid • ↑↑ release of thyroxin ↑↑ BMR • Abrupt onset • ↑↑ Temp 106 ↑↑ BP • ↑↑ Apical >200 Fatal arrhythmia's • Severe irritability/restlessness • Electrolyte imbalances • Vomiting • Delirium → coma → death
Therapy Medications • TylenolNo ASA (↑ T4 and T3 ) • MSO4 =↓ CNS & VS • Lugol’s Solution (SSKI) & PTU • ↓ vascularity and ↓ thyroxine • Cortisone↓ inflammation • Propranol↓ CO • ↓↓ Temp via Hypothermia blanket • O2 for ↑ BMR demands
Nursing Interventions Environment • Open windows & Keep away from heat • Frequent rest periods • Consistent routine and ↓ stimulation Diet • Meet metabolic needs • Small frequent meals • ↑ Protein, ↑ Carb, ↑ Calories • No Junk food!
Hypersecretion of Pituitary • Gigantism • 12 year old boy 6 ft 5 in • ↑↑ Growth via ↑↑ STH • ↑↑ muscles & viscera • ↑↑ ICP ↑↑ HA • Death @ age 30 • Cardiac unable to sustain CO • Therapy • Irradiation & Hypophsectomy
Hyposecretion of Pituitary Dwarfism (Vertically challenged) • Lesion, trauma or idiopathic • ↓ STH ↓ GH • ↓Growth < 10% • Disproportionate growth • Hands & feet short & chubby • adult male @ 4ft • Therapy • Surgery & Hormone Replacement • STH, ACTH, TSH, FSH, LH, MSH, • Thyroxin, Synthroid • Reinforce Age appropriate behaviors
Insulin Dependent Diabetes Mellitus Type I - IDDM Juvenile Onset • Genetic Predisposition or virus • causes an autoimmune process • destroys pancreatic insulin secreting B cells • ↓↓↓ Insulin Production • Glucose unable to enter the cells = Hyperglycemia • Glucose unavailable for cell metabolism = • cellular starvation
IDDM • Fatty Acids • Fats break down → fatty acids → Ketones • Ketones used as source of energy & release H++ • Metabolic Acidosis (Ketoacidois) • Remaining ketones accumulate in tissues • Excreted via urine (ketonuria) • Exhaled via lungs (Acetone/fruity breath) • Gluconeogenesis • Proteins break down ▲ to glucose in liver • ↑ Glucose circulating in blood → hyperglycemia
Clinical Signs • Polyphagia • ↑ appetite but unable to use glucose • Protein & lipid catabolism = body is starving!! • Muscle wasting with rapid weight loss = (–) N balance • Polyuria (enuresis is the 1st sign!!) • Glucose acts as a diuretic> Renal Threshold (180mg/100cc) • Excrete ↑ urine to removeglucose & ketones • ↑ Loss of electrolytes (Na+, Cl+, Ca+, Mg, PO4) • Polydipsia • ↑ Thirst due to polyuria • ↑ Intake > 2-3 Liters/day • Hyperglycemia • ↑ serum glucose • glucose adheres to vaginal wall = ↑ vaginal yeast infections
Diagnosis • Fasting Blood Sugar (FBS) >120mg/dl • May miss 85% early chemical diabetes • Post-prandial->150mg/dl • Eat ↑↑ carbohydrate meal (75-100 gm) • √ BS p 2H • Glucose Tolerance Test (GTT) > 200 • FBS & Urine S & A • Drink Glucola (75 gm carb) • √ BS & urine S & A q ½ H (x 4) • Glycosylated Hemoglobin (GHB, HbA1c) • Reflects BS for last 3-4 months • WNL 5.5 – 8 Poorly controlled >11.5 • Ketoacidosis >15
Treatment Insulin • ↑↑ Uptake & utilization of glucose by muscle & fat cells. Inhibits release of glucose in liver • Rapid Acting- Regular,Humulin R or Lispro • Onset 30 mins Peak 2-4H Duration 6-8H • Intermediate- NPH, Lente • Onset 2H Peak 6-8H Duration 12-16H • Long Acting- Ultralente, PZI • Onset 4-8H Peak 16-24H Duration 30-36H • Insulin Glargine-Lantus (rDNA origin) • Steady concentration over 24H No peaks. • Cannot be mixed with other insulin's
Insulin • Pediatric Dosages • Combination of Regular, NPH or Lantus 2 doses • AM (2/3 daily dose) ½ H a breakfast • PM (1/3 daily dose) ½ H a dinner • Administration • √ Brand √ Type • “clear to cloudy” 1st draw up Regular • SQ @ 90 angle • Rotate sites (Abd → Arms → Thighs) • Coverage • Based on BS (200-250 -2u R) • Additional regular insulin added to daily dose • Insulin Pump • Consistent coverage • No need for multiple daily injections • ↑ Independence & control • ↓ Ketoacidosis
Diet Therapy Maintain adequate calories for growth spurt. Need food for metabolism with insulin • NCS = No Concentrated Sweets & ↓ fats • ADA exchange diet • 3 meals + 3 snacks/day • ↑ Flexibility c exchanges 75 kcal = 1point • Meal planning • Consider school, activities & sports • Pt. preferences • Exercise • ↑ food intake 10-15gm complex carbs • for q 30 mins activity
Patient Teaching • Essential for optimal health • ↑ knowledge ↑compliance ↑control ↑health • Short sessions 15 -20 mins • Practice using equipment/supplies a D/C • Pathophysiology • S/S & Therapy • Long term sequella: • ↑ Infections, Retinopathy, Glomerulonecrosis, ↑ BP • Separate teaching for Pt & Family • Adolescents need to be empowered and independent
Hypoglycemia (Insulin Shock) ↑ Insulin ↓ Food ↑ Exercise • Rapid Onset • Sympathetic NS activated (Cool & Clammy) • Hungry, irritable, tremors, dizzy • Diaphoresis, pale skin, flushed cheeks • HA, blurred vision, slurred speech, • ↑ HR, shallow respirations, seizures • Therapy √ BS q 15 mins • Mild: milk or OJ • Moderate: Simple sugar (Lifesaver) • Severe: Glucagon IM/IV
Ketoacidosis (Diabetic Coma) ↑ Food ↑ Stress/Infection ↓Insulin • Gradual onset days – weeks • Kussmaul’s Respirations • Deep & rapid sighing breaths • Exhale = release ↑CO2, H+ = ↑ pH • Acetone Breath (fruity, sweet odor) • Metabolic Acidosis:↓ pH ↓ HCO3 ↓ PO2 • Hyperkalemia ↑ K+ • K+ follows glucose from cells → blood • Muscle weakness & Cardiac arrhythmias • Dehydration (Hot & Dry) • ↑ Temp, skin hot & dry, lethargic, mallar flush • ↓ Turgor & sunken eyeballs
DKA Therapy • ICU & NPO • √ V/S & BS Continuously • C/R monitor √ arrhythmias • Pulse ox & ABG • √ Neuro for cerebral edema • Electrolytes (√ K+) • Rebound Hypokalemia • K+ follows glucose → cells • √ I & O • IV NaCl & Regular Insulin (0.1u/kg)IVPB • NaHCO3 IVPB for metabolic acidosis • Constantly assess Pt’s response to RX!