Download
1 / 28
280 likes | 770 Views
Minimal change disease and treatment with steroids . 7/24/2007 Zae Kim, MD. Clinical Question. Why does MCD respond to steroid? Why do they develop resistance?. Introduction. Most common cause of the nephrotic syndrome in children

E N D
Minimal change disease and treatment with steroids 7/24/2007 Zae Kim, MD
Clinical Question • Why does MCD respond to steroid? • Why do they develop resistance?
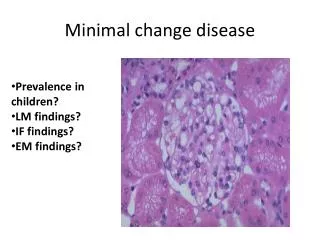
Introduction • Most common cause of the nephrotic syndrome in children • ~10-15% of nephrotic syndrome in adults, third most common after MN and FSGS • More common in Hispanics, Asians, Arabs and Caucasians • clinical and pathologicalentity defined by selective proteinuria and hypoalbuminemiathat occurs in the absence of • cellular glomerular infiltratesor • immunoglobulin deposits
Immunofluorescence Microscopy www.gamewood.net/rnet/renalpath/noimcx.jpg
The glomerular capillary wall Normal MCD Van den Berg, Weening, Clinical Science (2004) 107, 125–136
Pathogenesis - “Intrinsic factor” • Genetic basis for hereditary NS • NS of the Finnish type • Autosomal-recessive steroid-resistant NS • Familial forms of FSGS • Diffuse mesangila sclerosis associated with Denys-Drash syndrome and with Frasier syndrome • NS associated with nail-patella syndrome • Help elucidate molecular aspect of FSGS • Not clear for MCD
Molecular anatomy of the podocyte foot process cytoskeleton Nature Genetics24, 333 - 335 (2000)
Pathogenesis – extrinsic factor, better explanation for MCD • Clinical Observations - Shalhoub’s hypothesis • MCD frequently remits with measles infection • Corticosteroids and alkylating drugs cause a remission • Association of MCD with Hodgkin disease • Experimental Observations • T cell hybridoma (Koyama KI 1991 (40): 453-460) • Removal of glomerular permeability factor leads to normal kidney (Ali Transplantation 1994 Oct 15;58(7):849-52) • “circulating factor” • possible link between T-cell response and glomerular disease
How does steroid work in MCD? • Widely used in treatment but their mode of action is poorly understood • What is its effectiveness in MCD where there is no evident inflammation
Steroid – quick overview • Inhibitory effects on both innate and acquired immunologic function • Innate Immune function • Reduced Inflammatory response: • inhibit transmigration of leukocytes • attenuate the generation of inflammatory exudates • Phospholipase A2 suppresion • COX-2 suppression • Acquired Immune function • Antigen presenting cells, B cell and T cells
Direct effects of dexamethasone on human podocyte – Xing, Saleem, et al • Hypothesis: • Glucocorticoid exert direct protection of podocytes from injury and/or promotion of repair • Nephrin: podocyte specific protein • mutation of NPHS2 gene - cause congenital nephrotic syndrome of Finnish type • Studies show possible downregulation of nephrin in MCD
Result – effects of dexamethasone on podocyte maturation at 37 C and expression of nephrin Immunofluorescent staining Quantificaton of nephrin
Summary • Dexamethasone enhanced and accelerated podocyte maturation, with a particulary striking effect on expression of nephrin
Overexpression of Interleukin-13 Induces Minimal-Change–Like Nephropathy in Rats • Background • MCD may be a T cell dependent disorder that results in glomerular podocyte dysfunction • Th2 cytokine bias in patients with MCD • MCD associated with atopy and allergy • Relapse MCD with elevated IL-4 and IL-13 • Association between MCD and Hodgkins’s disease • IL-13 known to be an autocrine growth factorfor the Reed-Sternberg
Hypothesis • IL-13 may play an important role in the development ofproteinuria in MCNS by exerting a direct effect on podocytes,acting through the IL-13 receptors on the podocyte cell surface,initiating certain signaling pathways that eventually lead tochanges in the expression of podocyte-related proteins (nephrin, podocin, and dystroglycan) • IL-13 transfected mouse was used as a model
Comparison of control, IL-13-transfected mouse at experiment end (day 70) Yellow = p <0.001 vs control Red = p<0.001 vs control and Grp 1
Histopathologic features on day 70 at killing(A) Glomerulus of IL-13–transfected rat showing no significant histologic changes (periodic acid-Schiff stain). (B) Glomerulus of IL-13–transfected rat showing fusion of podocyte foot processes (arrows). (C) Glomerulus of control rat showing normal individual podocyte foot processes along the glomerular basement membrane (GBM; arrows).
Control IL-13 infected Immunofluorescence staining of glomeruli for protein expression of nephrin, podocin, dystroglycan, and synaptopodin nephrin podocin dystroglycan synaptopodin
Summary • IL-13-transfected rats • Developed minimal change like GN, as evidence by LM and EM changes • decrease in the expression of nephrin, podocin,and dystroglycan associated with increased urinary albumin excretion and podocytefoot process effacement • suggesting that these proteins areessential in maintaining the filtration barrier, thus controllingglomerular permeability • decrease was not due to loss ofpodocytes -
What does it all mean… • There is more to steroid than I knew… • “circulating factor” • Prognostic indicator? • Why are some MCDs steroid responsive while others are resistant?