Download

1 / 56

E N D
Quality control in serology Dr.T.V.Rao MD Dr.T.V.Rao MD
Process or system for monitoring the quality of laboratory testing, and the accuracy and precision of results Routinely collect and analyze data from every test run or procedure Allows for immediate corrective action What is Quality Control? Dr.T.V.Rao MD
Quality Control- QC refers to the measures that must be included during each assay run to verify that the test is working properly. Quality Assurance - QA is defined as the overall program that ensures that the final results reported by the laboratory are correct. “The aim of quality control is simply to ensure that the results generated by the test are correct. However, quality assurance is concerned with much more: that the right test is carried out on the right specimen, and that the right result and right interpretation is delivered to the right person at the right time” Definitions Dr.T.V.Rao MD
Quality Assessment- quality assessment (also known as proficiency testing) is a means to determine the quality of the results generated by the laboratory. Quality assessment is a challenge to the effectiveness of the QA and QC programs. Quality Assessment may be external or internal, examples of external programs Definitions Dr.T.V.Rao MD
Designing a QC Program – • Establish written policies and procedures • Corrective action procedures • Train all staff • Design forms • Assure complete documentation and review Dr.T.V.Rao MD
The Quality System Organization Personnel Equipment Process Control (QC & EQA) & Specimen Management Purchasing & Inventory Occurrence Management Assessment Documents & Records Process Improvement Customer Service Facilities & Safety Information Management Dr.T.V.Rao MD
The Quality Assurance Cycle Pre-Analytic Patient/Client Prep Sample Collection Personnel Competency Test Evaluations Reporting • Data and Lab Management • Safety • Customer Service Post-Analytic Sample Receipt and Accessioning Record Keeping Sample Transport Quality Control Testing Analytic Dr.T.V.Rao MD
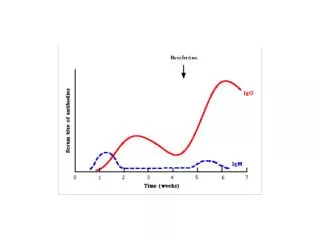
Need for Serological Tests • SEROLOGICAL TESTS are performed to demonstrate antigens in the serum, or the response of the human body to these infectious agent ( Antibodies ) to establish its contact with the immune system. Their diagnostic importance stems from demonstration of a rising titre of antibodies to the agent which inter alia indicates a progressive infection. In rare instances is the presence of antibody in a single sample indicative of infection and disease. Serological tests are of importance in epidemiological studies and to ascertain the response of the population to vaccines and other immunopotentiators. Dr.T.V.Rao MD
Importance of Serological Tests • Serological tests are of importance in epidemiological studies and to ascertain the response of the population to vaccines and other immunopotentiators. Dr.T.V.Rao MD
Serology performed mainly as vitro tests • Serological tests are also useful for the in vitro detection of microbial infections, and for the classification and sub classification of infectious agents (e.g. Salmonella, Shigella, Streptococcus, etc.). Dr.T.V.Rao MD
COLLECTION OF SPECIMEN • There must be a system for the orderly and efficient requesting of tests; collection and identification of specimens; and transporting, preparation, and storage of specimens. Nothing is more important than having an adequate amount of an appropriate specimen in good condition for examination. If each specimen is not properly collected, labeled, and handled, or is not representative, the laboratory may do more harm than good by testing it. Dr.T.V.Rao MD
Haemolysed specimens are not suitable for testing • Haemolysed blood specimens are not suitable for serological studies. It is always advisable to avoid factors which cause hemolysis (Table 14.1). Specimens containing precipitates should be centrifuged prior to testing. Dr.T.V.Rao MD
Avoidable causes of hemolysis • Blood sampling through too small bore of a needle • Forced suction of blood in the syringe during blood collection • Vigorous shaking of blood from the syringe, especially through a needle • Centrifuging blood sample at a high speed before clotting • Freezing and thawing of blood • Unclean tubes with residual detergents Dr.T.V.Rao MD
Serology can Detect either antigen or antibody • Serological reactions detect either a specific antigen produced by the microorganism or a specific immune response of the human body. Serological tests may detect: • 1 an immunological principle (antigen-antibody reaction: ELISA, Widal) • 2 a non-specific reaction (VDRL test) • 3 a reaction mediated by complement (complement fixation test) Dr.T.V.Rao MD
advantages with serological methods. • Rapid identification of agent • High specificity of detection of antigen • Simplicity of performance • Safe procedures • Diagnostic aids • Epidemiological tools • Retrospective confirmation of diagnosis Dr.T.V.Rao MD
List of tests added every day • A wide variety of serological tests are now available and every day new ones are added to an already impressive list. Every laboratory must define a policy for conducting these tests because some may be expensive, all require certain reagents (sera or antigens etc.) which have limited shelf life, and all require standardised techniques which must be documented in SOPM. Dr.T.V.Rao MD
Standard operating procedures are foundations in all protocols • An important element in maintaining day-to-day uniformity in laboratory results is an established procedure manual (SOPM) which details all phases of the laboratory’s operation (including safety precautions) and is used by all laboratory personnel. It should include instructions for collecting, transporting, and storing specimens, for preparing and storing reagents, and for performing tests. In addition, the controls and calibrators to be used should be listed along with directions for their use, expected results, and instructions for corrective measures if the expected results are not obtained. Dr.T.V.Rao MD
Control Sera • Source • Some control sera are available commercially. Small volumes are generally available as components in kits but are intended to be used only with a single kit. A few may be available in larger quantities. • Preparation • Sera to be used as controls should be kept sterile to avoid deterioration. In general each procedure should have a normal control serum (negative), a strong positive control serum, and another positive control serum which is reactive at the critical concentration (borderline positive). With some tests, controls with a low concentration of analyze should be included. Controls recommended by the manufacturer of a particular test should always be used and additional control sera can be included if a test involves special problems. Dr.T.V.Rao MD
Storage • Sera to be used as controls should be standardized against international reference materials when they are available. "Standards" included in commercial kits are not calibrated with each other and often are not interchangeable. These should be stored in aliquotes in frozen forms. Repeated freezing and thawing should be avoided. Dr.T.V.Rao MD
Quality reagents give optimal results • Quality reagents are necessary for quality performance. A record should be kept of any changes in reagents in case the performance of a test changes. Before new reagents are introduced into a system they should be tested in parallel with the old reagents against a panel of appropriate reference sera to be sure that consistent reactions are obtained. The results obtained with the panel should reflect the sensitivity and specificity of the reagents being compared. Dr.T.V.Rao MD
Label all the reagents • Reagents should be clearly labeled to indicate their identity, hazards involved in their use, recommended storage conditions, and preparation and expiration dates. Dr.T.V.Rao MD
EQUIPMENT AND INSTRUMENTS • All glassware used in immunologic tests must be clean and free of detergent. Chipped or etched glassware should be discarded. Calibrated glassware should be checked for accuracy. • The user’s accuracy and precision requirements should be met or exceeded when equipment is tested under working conditions. The manufacturer’s specifications for performance should be checked and met. Instruments and equipment should be monitored routinely. The temperature of water baths, incubators, refrigerators, and freezers should be checked periodically and records maintained. Maintenance should be performed and records kept on a regular basis by individuals who are trained and are familiar with the equipment. Dr.T.V.Rao MD
Quality control of instruments • Instruments used for measurements including spectro-photometers, spectrometers, dilutors, and automatic pipettes should be calibrated on a regular basis. Dr.T.V.Rao MD
Selecting a procedure or a protocol Dr.T.V.Rao MD
Choose the appropriate test to your laboratory • As new tests and methods are developed for various analytes (antibodies or antigens), the most appropriate must be chosen for each laboratory’s needs. A number of factors must be considered, including bias, specificity, sensitivity, precision, cost and ease of performance. Bias, specificity and sensitivity may be related. Frequently the more sensitive a test, the less specific it is. Bias may result from low specificity or sensitivity. Dr.T.V.Rao MD
How to reduce the presence of Bias • To determine the presence of bias, the proposed method should be compared with other reliable methods, preferably with a standard method or clinical data. The same specimens should be run with both methods in the same laboratory and the results compared, although interlaboratory comparisons are also useful. If the results from the different methods do not agree, one must determine the reason for the difference and then decide which result is more useful. Dr.T.V.Rao MD
What is clinical specificity • The clinical specificityof a method is evaluated by testing negative samples and samples containing substances which might cause interference. Closely related or cross-reacting substances frequently found in clinical specimens should be included. Dr.T.V.Rao MD
Making Suitable Dilutions 100 ul serum in tube 1 Mix and Transfer Discard 100ul diluent in each tube Each tube is a 1:2 dilution of the previous tube Dr.T.V.Rao MD
2 4 8 16 32 64 128 256 512 1024 2048 4096 8192 16384 32768 65536 131072 262144 524288 Selecting a Suitable Sample Dilution Serial Dilutions on Abbott AxSYM HIV-1/HIV-2 MEIA 20 18 16 14 12 S/Co Ratio 10 8 6 Pos Cont 3.3 4 Cut Off 1.0 2 Neg Cont 0.38 0 Doubling Dilutions Dr.T.V.Rao MD
What is clinical Sensitivity • The clinical sensitivity of a method being evaluated should be compared to that of other methods, but the purpose of the test must also be considered. In general, a definitive test need not be as sensitive as a screening test. The test should distinguish between normal and abnormal levels of analyze. Dr.T.V.Rao MD
Evaluation on precision • The precision of a quantitative or Semiquantitative test must be evaluated in light of the precision required for the clinical application of the test results. Many factors affect precision, but one that is frequently overlooked in serologic tests is the size of the dilution increments. If all other variables are held constant, serologic tests tend to become less precise as the size of the dilution increment increases. For example, it should be expected that a test based on a four fold dilution would be less precise than the same test with a two-fold dilution. Dr.T.V.Rao MD
True value- this is an ideal concept which cannot be achieved. Accepted true value - the value approximating the true value, the difference between the two values is negligible. Error- the discrepancy between the result of a measurement and the true (or accepted true value). Errors in measurement Dr.T.V.Rao MD
When you need a highly sensitive test • A test with maximum possible sensitivity is desirable when a disease is serious and its diagnosis should not be missed when the disease is treatable, and when false-positive results do not lead to serious problems. Similarly a test with maximum specificity is desirable when a disease is serious but is not treatable, the knowledge that the disease is absent has psychological or public health value, and false-positive results can lead to serious problems. A high predictive value of a positive test result is desirable when treatment of a false positive might have serious consequences. Dr.T.V.Rao MD
Quality control of tests detecting antibodies • The performance of tests is monitored with controls. Antigenic serum panels as well as sera with known quantities of antibodies are available and should be routinely used. Correct performance of reagents is reflected by the expected reaction in tubes which lack one or more of the components necessary for the reaction. For example, the presence of anti-streptolysin O reagent is demonstrated by haemolysis in the tube containing the reagent buffer and cells but no antibody to inhibit haemolysis. Dr.T.V.Rao MD
Antibody test • Flocculation test(RPR) • control procedures required • Nonreactive serum controlWeakly reactive serum controlReactive serum control • Expected results • No clumpingClumping of graded activityClumping of graded activity Dr.T.V.Rao MD
Antibody test • Antibody test • Latex agglutination test(ASO) • Control procedures required • Negative control serumPositive control serum • Expected results • No clumpingClumping Dr.T.V.Rao MD
Antibody test • Antibody test • Direct agglutination(Widal test, STA for Brucellosis) • Control procedures required • Antigen controlNegative control serumPositive control serum • Expected results • No clumpingNo clumpingClumping Dr.T.V.Rao MD
Antibody test • Antibody test • Passive haemagglutination (ASO) • Control procedures required • Streptolysin controlRed cell control • Expected results • HemolysisNo hemolysis Dr.T.V.Rao MD
Antigen test • Antigen test • Coagglutination test(Haemolytic streptococci meningitis antigens) • Control material • Group A,B,C streptococciN.meningitidis • Expected result • Agglutination with corresponding serum, Dr.T.V.Rao MD
Quality control procedures for tests detecting antigens • Antigen test • capsular Quelling reaction(Omni serum, H.influenzae type b) • Control material • PneumococciHaemolytic streptococciH.influenzae type bAcinetobacter anitratum • Expected result • Capsular swellingNo reactionCapsular swellingNo reaction Dr.T.V.Rao MD
REPORTING AND RECORD KEEPING • Complete and accurate records must be maintained in a good quality assurance programme. These records should include personnel information; details of equipment, preventive maintenance, service, and repair; copies of reports to physicians or other clients; accession records; records of reagents and materials used; records of observations made concurrently with the performance of each step in the examination of specimens; proficiency testing results; and internal quality control results. Dr.T.V.Rao MD
The degree of fluctuation in the measurements is indicative of the “precision” of the assay. The closeness of measurements to the true value is indicative of the “accuracy” of the assay. Quality Control is used to monitor both the precision and the accuracy of the assay in order to provide reliable results. Accuracy and Precision Dr.T.V.Rao MD
Precision and Accuracy Dr.T.V.Rao MD Precise and inaccurate Precise and accurate
Establish written policies and procedures Corrective action procedures Train all staff Design forms Assure complete documentation and review Designing a QC Program – Dr.T.V.Rao MD
Quality control is performed for both, system is somewhat different Controls available Blood Bank/Serology/Micro RPR/TPHA Dipstick technology Pregnancy Qualitative QC Dr.T.V.Rao MD
Select appropriate controls Assay them repeatedly over time at least 20 data points Make sure any procedural variation is represented: different operators different times of day Determine the degree of variability in the data to establish acceptable range Establishing Control Ranges Dr.T.V.Rao MD
Measurement of Variability • A certain amount of variability will naturally occur when a control is tested repeatedly. • Variability is affected by operator technique, environmental conditions, and the performance characteristics of the assay method. • The goal is to differentiate between variability due to chance from that due to error. Dr.T.V.Rao MD
Input data required - such as standards used, calibration values, and values of physical constants. Inherent characteristics of the quantity being measured - e.g. CFT and HAI titer. Instruments used - accuracy, repeatability. Observer fallibility - reading errors, blunders, equipment selection, analysis and computation errors. Environment - any external influences affecting the measurement. Theory assumed - validity of mathematical methods and approximations. Sources of error Dr.T.V.Rao MD
Avoiding the errors • The accessioning and reporting system should minimize the possibility of clerical errors. Precautions should be taken to prevent reporting results on the wrong specimen and transposing digits in reporting quantitative data. The system should be so designed that the history associated with a sample can be reconstructed in detail if necessary. Who performed which tests, what reagents and lot numbers they used, what the control results were for that run, and how and when the results were reported should also be documented Dr.T.V.Rao MD
An error which varies in an unpredictable manner, in magnitude and sign, when a large number of measurements of the same quantity are made under effectively identical conditions. Random errors create a characteristic spread of results for any test method and cannot be accounted for by applying corrections. Random errors are difficult to eliminate but repetition reduces the influences of random errors. Examples of random errors include errors in pipetting and changes in incubation period. Random errors can be minimized by training, supervision and adherence to standard operating procedures. Random Error Dr.T.V.Rao MD