TIMACS: Timing of Intervention in Acute Coronary Syndromes
Learn about a randomized trial comparing early vs. delayed invasive strategies for ACS patients. Results show no significant difference in primary outcomes, but early strategy is superior for high-risk patients. Early intervention also decreases refractory ischemia risk by 70%.

TIMACS: Timing of Intervention in Acute Coronary Syndromes
E N D
Presentation Transcript
TIMACS Tim ing of Intervention in patients with A cute C oronary S yndromes An International Randomized Trial of Early Versus Delayed Invasive Strategies in Patients with Non-ST Segment Elevation Acute Coronary Syndromes Shamir R. Mehta MD On behalf of the TIMACS Investigators
Design, Eligibility Criteria and Protocol UA or NSTEMI 2 of 3 Criteria: Age > 60, ischemic EKG Δ or ↑ biomarker AND suitable for revascularization Excluded Contraindication for LMWH or high risk of bleeding or not a suitable candidate for revascularization ASA, clopidogrel, GP IIb/IIIa antagonist as per routine practice RANDOMIZE* Early Invasive Coronary angiography as soon as possible followed by PCI or CABG (no later than 24 hours) Delayed Invasive Coronary angiography any time >36 hrs followed by PCI or CABG *Center chose randomization ratio 1:1, 1:2 or 2:1 Early: Delayed
Outcomes • Primary • Composite of Death, new MI or Stroke at 6 mo. • Secondary Composite of: • Death, new MI or refractory ischemia • Death, new MI, stroke, refractory ischemia or repeat revascularization • Stroke
Primary OutcomeDeath, MI, or Stroke Death/MI/Stroke at 180 days Delayed Early 0.10 Cumulative Hazard 0.06 HR 0.85 95% CI 0.68-1.06 P= 0.15 0.02 0.0 0 30 60 90 120 150 180 Days No. at Risk Delayed 1438 1328 1269 1254 1234 1229 1211 Early 1593 1484 1413 1398 1391 1382 1363
Death/MI/RI at 180 days Delayed 0.12 Early 0.08 Cumulative Hazard 0.04 0.0 0 30 60 90 120 150 180 Days No. at Risk Delayed 1438 1303 1243 1230 1209 1205 1187 Early 1593 1485 1417 1402 1394 1386 1366 Secondary OutcomeDeath, MI, or refractory ischemia HR 0.72 95% CI 0.58-0.79 P=0.002
Delayed 0.20 Early 0.15 Cumulative Hazard 0.10 0.05 0.0 0 30 60 90 120 150 180 Days No. at Risk Delayed 1438 1250 1166 1150 1128 1118 1097 Early 1593 1400 1321 1304 1287 1276 1256 Secondary OutcomeDeath, MI, stroke, RFI or Rep Intervention Death/MI/RI/Stroke/Rep Int at 180 days HR 0.84 95% CI 0.71-0.99 P=0.039
GRACE Risk Score: Primary Outcome HR 0.65 95% CI 0.48-0.88 P=0.005 Death, MI or Stroke at 6 mo. Interaction P=0.0097 HR 1.14 95% CI 0.82-1.58 P=0.43 Low/Int Risk GRACE Score < 140 N=2070 High Risk GRACE Score >= 140 N=961
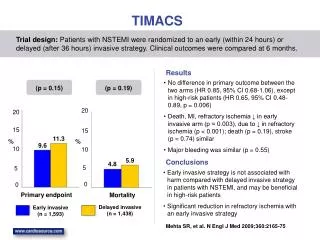
Conclusions • Overall, we found no significant difference between an early and a delayed invasive strategy for prevention of death, MI or stroke (primary outcome). • However, in the subgroup at highest risk (GRACE score > 140), an early invasive strategy was superior to a delayed invasive strategy for prevention of death, MI or stroke • Early invasive strategy also had a large impact on reducing the rate of refractory ischemia by 70%. • There were no significant differences in major bleeding or other safety concerns between the two strategies
Implications • Most patients with ACS can be managed safely with either an early or a delayed invasive strategy • In a subset of patients at highest risk (GRACE score>140), early intervention is superior and these patients should be taken to the cath lab early • In all other patients, the decision regarding timing of intervention can depend on other factors, such as cath lab availability and economic considerations.