从 TIMACS 研究结果再议 NSTEACS 介入时机
从 TIMACS 研究结果再议 NSTEACS 介入时机. 福建医科大学附属协和医院心内科 福建省冠心病研究所 陈良龙 MD PhD FACC. NSTE-ACS : Pathogenesis. Vulnerable Plague Not totally occlusive thrombosis White thrombus. Yeghiazarians Y, et al. N Engl J Med. 2000;342:101-114. 背景. 早期 尽早造影,明确病变,对后续治疗策略有指导意义; 减少等待期间不良事件的发生 [1] ; 缩短住院时间。

从 TIMACS 研究结果再议 NSTEACS 介入时机
E N D
Presentation Transcript
从TIMACS研究结果再议NSTEACS介入时机 福建医科大学附属协和医院心内科 福建省冠心病研究所 陈良龙 MD PhD FACC
NSTE-ACS:Pathogenesis • Vulnerable Plague • Not totally occlusive thrombosis • White thrombus Yeghiazarians Y, et al. N Engl J Med. 2000;342:101-114.
背景 • 早期 • 尽早造影,明确病变,对后续治疗策略有指导意义; • 减少等待期间不良事件的发生[1]; • 缩短住院时间。 • 延迟 • 在积极抗血小板、抗凝、稳定斑块等治疗基础上,介入治疗并发症少,安全系数更高 [2]; • 等待期间可能发生不良事件乃至死亡; • 延长住院时间/增加费用。 1.Neumann FJ, et al JAMA 2003;290:1593–9. 2.Smith SC et al. Circulation 2001;103:3019–41.
目前指南I类推荐指征 • UA/NSTEMI 患者,若有下列情况应早期介入 • 具有任何高危因素 • 病变适合PCI • 无影响PCI的严重合并症
问题与焦点 • 介入治疗的最佳时机尚不确定 • 早期:多早? • 延迟:多长? • 哪些患者需要尽早治疗?要多早? • 目前的RCT研究结果不一致[1,2]。 1.Neumann FJ, et al JAMA 2003;290:1593–9. 2. Riezebos RK, et al. Heart 2009;95:807-12.
Timing of Intervention in Patients with Acute Coronary Syndromes(TIMACS)
Endpoint • Primary endpoint • composite of death, MI, stroke at 6 m. • Secondary endpoints • composite of death, MI, refractory ischemia at 6m. • composite of death, MI, stroke, refractory ischemia, repeat revascularization at 6m.
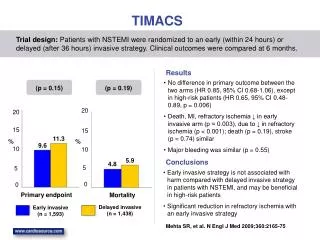
Primary and secondary outcomes in TIMACS, early vs delayed strategies *Primary end point Mehta SR, et al. N Engl J Med 2009;360:2165-75.
Rates of death, MI, or stroke within six months according to GRACE score *Low/intermediate risk=GRACE score <140 High risk=GRACE score >140 *Prespecified analysis
Kaplan–Meier Cumulative Risk of the Primary Outcome Stratified According to GRACE Risk Score High risk >140 Low-to- intermediate risk ≤140 High risk:>140; Low-to-intermediate risk: ≤140.(GRACE Risk Score)
Conclusion • 与延迟干预相比,早期干预对于NSTE-ACS患者6个月不良事件发生率没有显著差异; • NSTE-ACS患者接受早期干预安全性良好; • 高危患者(GRACE评分>140)可从早期干预策略获益; • 早期干预可显著减少NSTE-ACS患者再发心绞痛的发生率,且不增加出血风险;
其他随机临床试验 • ABOARD • ISAR-COOL • OPTIMA
Trial Flow: ABOARD Primary endpoint Peak troponin value during hospitalization Second endpoint Death, MI, urgent revascularization, or recurrent ischemia at 1m Montalescot G, et al. JAMA 2009;302:947-54.
ABOARD研究结果 Montalescot G, et al. JAMA 2009;302:947-54.
结论 • 对于NSTE-ACS患者, 即刻(1小时)与延迟(次工作日)介入治疗策略比较 • 不能减少肌钙蛋白定义的MI • 不能减少1个月时的死亡、MI、紧急血运重建或 复发心肌缺血 Montalescot G, et al. JAMA 2009;302:947-54.
Trial schema: ISAR-COOL Endpoint: death, MI at 30d
ISAR-COOL研究结果 • This outcome was attributable to events occurring before catheterization; • after catheterization, both groups incurred 11 events each (P=.92). Neumann FJ, et al JAMA 2003;290:1593–9.
结论 • 对于不稳定ACS患者, 与早期介入治疗+强化抗血小板比较, • 延迟介入治疗+延长抗栓治疗并不能改善临床结局(死亡、MI), • 相反地,后者在等待期增加了约50%的事件。 Montalescot G, et al. JAMA 2009;302:947-54.
Trial schema: OPTIMA Endpoint: death, MI, at 30d and 6m Riezebos RK, et al. Heart 2009;95:807-12.
OPTIMA研究结果* • *No deaths occurred in either group Riezebos RK, et al. Heart 2009;95:807-12.
结论 • 对于NSTE-ACS患者,与延迟介入治疗(24-48H)比较: • 尽管有强化的抗栓治疗,早期介入治疗(24H)还是增加MI • 对于非顽固NSTE-ACS患者,介入治疗至少应延迟至入院后24H进行 Montalescot G, et al. JAMA 2009;302:947-54.
4 RCTs总结 • For Pts with high risk, • too early or too late intervention is harmful. • 24 h may be the proper time window in setting of intensive antithrombotic therapy
The Answers • 多早? • 在有效抗栓基础上, • 约在入院后24H,是早期PCI的最佳窗口 • 哪些患者早做? • 高危者(包括血流动力学不稳定\恶性心律失常) • 无禁忌者
Fighting CVD U U 感 谢!
Reconsideration of Interventional Therapeutic Time Window for NSTE-ACS——Hint from the Result of TIMACS Chen Lianglong MD, PhD, FACC Cardiology, Union Hospital, Fujian Medical University
NSTE-ACS:Pathogenesis • Vulnerable Plague • Not totally occlusive thrombosis • White thrombus Yeghiazarians Y, et al. N Engl J Med. 2000;342:101-114.
Background • Early intervention might prevent ischemic events that could occur while the pts are awaiting a delayed procedure. • Alternatively, by treating pts with intensive antithrombotic therapy and delaying intervention for several days, procedure-related complications might be avoided with intervention on a more stable plaque.
Current CLASS-I recommendations • An early invasive strategy is indicated for pts with UA/NSTEMI • who have any of the high-risk features & • who have coronary lesions amenable to PCI & • who have no serious comorbidities.
Uncertain • the optimal timing of such intervention remains controversial. • Early strategy: how early • delayed strategy: how prolonged
Timing of Intervention in Patients with Acute Coronary Syndromes (TIMACS)
Endpoint • Primary endpoint • composite of death, MI, stroke at 6 m. • Secondary endpoints • composite of death, MI, refractory ischemia at 6m. • composite of death, MI, stroke, refractory ischemia, repeat revascularization at 6m.
Primary and secondary outcomes in TIMACS, early vs delayed strategies *Primary end point Mehta SR, et al. N Engl J Med 2009;360:2165-75.
Rates of death, MI, or stroke within six months according to GRACE score *Low/intermediate risk=GRACE score <140 High risk=GRACE score >140
Kaplan–Meier Cumulative Risk of the Primary Outcome Stratified According to GRACE Risk Score High risk >140 Low-to- intermediate risk ≤140 High risk:>140; Low-to-intermediate risk: ≤140.(GRACE Risk Score)
Conclusions • Early intervention did not differ greatly from delayed intervention in preventing the primary outcome. • but it did reduce the rate of the composite secondary outcome of death, myocardial infarction, or refractory ischemia • and was superior to delayed intervention in high-risk patients.
Other RCTs • ABOARD • ISAR-COOL • OPTIMA
Trial Flow: ABOARD Primary endpoint Peak troponin value during hospitalization Second endpoint Death, MI, urgent revascularization, or recurrent ischemia at 1m Montalescot G, et al. JAMA 2009;302:947-54.
ABOARD-Results Montalescot G, et al. JAMA 2009;302:947-54.
Conclusion • In pts with NSTE-ACS, a strategy of immediate intervention compared with a strategy of intervention deferred to the next working day (mean,21h) did not result in a difference in MI as defined by peak troponin level. Montalescot G, et al. JAMA 2009;302:947-54.
Trial schema: ISAR-COOL Endpoint: death, MI at 30d
ISAR-COOL:Results • This outcome was attributable to events occurring before catheterization; • after catheterization, both groups incurred 11 events each (P=.92). Neumann FJ, et al JAMA 2003;290:1593–9.
Conclusion • In pts with unstable coronary syndromes, deferred intervention for prolonged antithrombotic pretreatment does not improve the outcome compared with immediate(early) intervention accompanied by intense antiplatelet treatment.
Trial schema: OPTIMA Endpoint: death, MI, at 30d and 6m Riezebos RK, et al. Heart 2009;95:807-12.
OPTIMA: Results* • *No deaths occurred in either group Riezebos RK, et al. Heart 2009;95:807-12.