Download
1 / 53
740 likes | 2.13k Views
Patellofemoral Osteoarthritis. March 3, 2012 New England Baptist Hospital AORN Anthony Schena, MD. DISCLOSURES. Who. Patellofemoral Joint. Articulation between the patella and the trochlea Trochlea designed to prevent lateral subluxation

E N D
Patellofemoral Osteoarthritis March 3, 2012 New England Baptist Hospital AORN Anthony Schena, MD
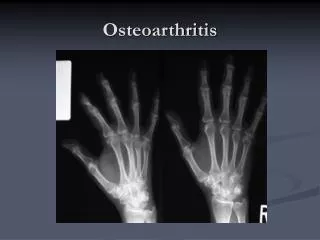
Patellofemoral Joint • Articulation between the patella and the trochlea • Trochlea designed to prevent lateral subluxation • Soft tissue structures assist/prevent this as well • VMO Tethers to the ITB/VL/VMO • MPFL • Medial retinaculum • Patella has the thickest cartilage in the body • Forces approach 7 x body weight with routine exercises
Patella • Increases the strength of the quad • ½ body wt with level walking • 3.3 x wt with stairs • From 0-90 ° pressure goes from inf to sup pole • Odd facet engaged at 110°
Pathophysiology of Disease • Causes of trauma to the PF joint • Acute • Direct impact-dashboard • Fracture • Dislocation • Tendon rupture • Chronic • Overload with activities • Weight • Lower limb Malalignment • OCD
Direct Impact/Contusion • Damages cartilage along PF joint • Gradual wearing down vs acute cartilage defect • Treat acute chondral loss if possible • Surgically repair • ACI/OATs • ? Offload
Fracture • If displaced, treat surgically • Need anatomic alignment • Can still breakdown over time • ? Pain from hardware
Dislocation • One time vs chronic laxity • Stabilize Patella before damage becomes too severe • Even with cartilage breakdown, need to stabilize joint
Weight/activities • Increases dramatically with activities that stress the patellofemoral joint (up to 7-8 x body wt) • Stairs, squatting, kneeling, walking/hiking downhill • Modest weight loss can be helpful • Change activities • Address other lower extremity issues
Lower Extremity Malalignment • Pes Planus (flat feet) • Tibial torsion • Genu valgum (knocked knees) • Hypoplastic lateral trochlea • Excessive femoral anteversion • Weak hip abductors/External rotators
Miserable Malalignment Internally rotated hips Genu valgum Hyperpronation/flat feet
Physical Exam • History: repetitive overuse vs acute event/trauma • Ask about old MVA, sports injuries, instability episdoses, daily activities that cause pain, treatments that make the pain better (did they take NSAIDs the day of the exam) • Exam: • Hips to toes • In shorts, both knees exposed • Gait analysis before or after exam while in shorts
Exam • Hips • ROM/flexibility • ITB, abductors, adductors, flexors, extensors, ERs • OBER test • Muscular strength
OBER TEST • Test ITB
Exam • Knee • ROM • Effusion/swelling/general appearance • Flexibility • Prone Quad • Also good check for femoral anteverion-knee flexed to 90 and IR until greater Trochanter is Maximally prominent laterally • Muscular Tone/symmetry • VMO • Balance • Thigh Circumference • Extensor lag/VMO lag
Patella • Mobility/translation-apprehension • Tenderness • Tracking through ROM • J sign • Tilt • Q angle • Normal at or less than 15 degrees • Position of the Tibial tubercle
What are the other issues • Concomitant disease in the medial or lateral joint in a patient >50…most likely will lead to a TKA • With intact menisci, could consider a resurfacing of the involved compartment and the PF joint
Isolated Patellofemoral OA • Location of Disease • Entire patella versus certain quadrant • Age • History/Exam • Pain with stairs/squatting • Effusions • Crepitus • Activity level
Imaging • X-rays • Merchant View • Tilt • CT scans • MRI • Subchondral cysts/cartilage loss
Treatment • Non-operative • NSAIDs • Strengthening • VMO/Closed Chain • Patella tracking braces • Activity modification • Weight loss • Viscosupplementation • Cortisone
Arthroscopy • Debride damaged cartilage • Lavage knee • Schonholtz/Long-49% G/E at 40 months • Federico/Reider – 58% traumatic/41% atruamatic G/E • +/- lateral release • Isolated patella or trochlear lesions • Microfracture/abrasion chondroplasty
ACI • Controversial • Poor long term studies • Most patients poor candidates due to chronicity of disease and degenerative changes to the underlying bone (cystic changes) • When considered, need to address the underlying malalignment • Off load the patellofemoral joint
Tibial Tubercle Osteotomy • Unloads the Patellofemoral joint • Can Correct Malalignment • Useful for patients with articular damage to the lateral and inferior patella (AMZ) and the entire patella (straight osteotomy)
Recovery • 6 weeks for osteotomy to heal • Can weight bear in brace • Start PROM • Once ambulatory-work on quad strength, balance, functional recovery • May still need to treat Effusions, anterior knee pain • Weight control • Activity modification
Patellofemoral Resurfacing • Replace patella cartilage loss with plastic component • Stryker Triathalon X3 patella vsinlay UHMWE polyethylene • Trochlear lesion replaced with inlay metal component • Cobalt-Chromium alloy • Titanium Stud • assssdsa Arthrosurface ™
ProSports Outcomes • 60 patients over four years • Three failures • One converted to a TKA • Two converted from first generation to second generation trochlear implant • One patient just 6 weeks out with tracking issue-no pain/very weak VMO May require further surgery