Electromagnetic navigation (Superdimensional bronchoscopy)
Electromagnetic navigation (Superdimensional bronchoscopy). Assoc. Prof. Can Sevinc Dokuz Eylul University School of Medicine Pulmonary Medicine Department Izmir - Turkiye. What is electromagnetic navigation?. “Mapquest”. “Lungquest”. From: A. Mehta. Who developed?. History.

Electromagnetic navigation (Superdimensional bronchoscopy)
E N D
Presentation Transcript
Electromagnetic navigation (Superdimensional bronchoscopy) Assoc. Prof. Can Sevinc Dokuz Eylul University School of Medicine Pulmonary Medicine Department Izmir - Turkiye
What is electromagnetic navigation? “Mapquest” “Lungquest” From: A. Mehta
History • superDimension, Ltd. • Israel, 1995 • For developing minimal invazive diagnostic tools for respiratory system diseases • The studies was started at 2001 again. • At 2003, • Initial results of the “superDimention Bronchus” clinical studies was declared • Professor Heinrich Becker, Thoraxklinik in Heidelberg, Germany
FDA approval; November 2004 • SD system was gained to our clinic at the end of 2005 • First case; 15 December 2005
SD indications ? • Peripheral lung lesions which can’t be seen and reached with conventional bronchoscopy • Especially the nodules and masses • You can reach the lesions by using the CT map guidance and real-time electromagnetic navigation • Biopsy and cytologic specimen can be taken • Histopathologic diagnosis chance
Components of the SD system • Main Processor • Two computers with special software • Spiral CT, DICOM • DICOM: The Digital Imaging and Communications in Medicine • Locatable guide • Working channel
Monitor PC Location Processor Location Board Location Amplifier Isolation Transformer
LOCATABLE GUIDE • A steerable cable which is put into the working channel of the bronchoscope by an adaptor and can reach the peripheral region of the lung where can be reached by bronchoscope. • It can follow the location and direction in real-time and 3 dimentionally by using the special sensor at the tip of the guide.
EXTENDED WORKING CHANNEL An apparatus which is put into the application canal of the bronchoscope and directed to the target lesion by using the Locatable Guide and also helps the bronchoscopic tools to reach to the target lesion.
LOCATION BOARD • A specially designed table that creates an electromagnetic area of very low frequency. • It is put under the back of the patient on the bronchoscopy table. • It is used for establishing the place of the Locatable Guide Sensor, in real time during the process.
SuperDimension Bronchus System • It reaches the tools (biopsy forceps, brush etc.) to the peripheral targets. • “3D CT mapping” is used for finding the way. • The device can establish and locate the place of the tools in “real time” and “3D”.
Preparation before the procedure • Multislice CT • 2.0-3.5 mm slice thickness, • 1.0-2.5 mm slice interval • Image type: original • Image diameters: 512 x 512 pixel, the whole chest imaging • Record of the digital data to CD.
Planning (approximately 10 min.) • A special computer programme. • Digital CT images are used. • At least 5-6 referance points are determined on the virtual broncoscopic images. • Target lesion(s) are marked and their diameters are measured. • The prepared planning file is recorded to the CD or USB disc.
MAIN CARINA RIGHT SUPERIOR LOBE RIGHT MIDDLE LOBE RIGHT INFERIOR LOBE LEFT SUPERIOR LOBE LEFT INFERIOR LOBE
Planning Loading of the CT images (DICOM) Choosing of the Registration Points Marking of the Target Points Loading and Transfer of Planning File
Procedure(approximateley 20 - 30 min.) • Cooperation of the digital video bronchoscopy system and SD system • FB with local anesthesia • If there is no visible endobronchial lesions, the SD process is started. • The locatable guide is opened.
Registration points established during the planning procedure is marked to the SD system by using the LG, before the procedure again. • Matching the points which • marked on the CT and • the points marked during the bronchoscopy.
LG is directed to the target lesion by watching the LG movements on the system screen 3D. • The match of the target is seen on the screen.
LG is pulled back. • Biopsy forceps is put into the working channel . • 3-5 biopsy sample is taken. • Brushing specimen can be taken if necessary. • Lavage is taken.
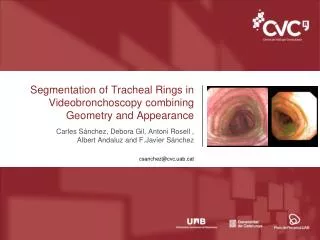
The tools are directed on the CT map in real-time by using the multiplane imaging.
Procedure (summary) Loading of Planning File Setup Registration Navigation
Planning Process Navigation Biopsy CT Scan DICOM CD
Mediastinal lymph node approach • There is no enough data yet. • According to the initial data of the experienced centers, it’s diagnostic value is high.
Which centers (in Turkiye) ?3 centers… (74 centers in world)
Experience of our clinic • Between 15 December 2005 – 30 November 2006 20 cases • Our diagnostic success rate is about 60% • At 30 November 2006; • The usage of the system is stopped by the company untill a second anouncement. • Because of the pneumothorax complication reported at a case in US.
ATS 2006Poster Presantation After 10 procedures, diagnostic yield is increased
ERS 2006Poster Presantation The SDBS enables a definitive diagnosis in 91% of lymph node cases. SDBS procedure has led to in 21 of the patients (73%) of peripheral lesions
Navigational bronchoscopy by electromagnetic guidance (superDimension; Plymouth, MN) is a groundbreaking concept in the diagnosis of peripheral lung lesions. • A preliminary study 58 has shown a diagnostic yield of 69% in 29 patients with lesions ranging in size from 12 to 106 mm in diameter and a mean distance to the pleura of 19.6 mm. • The overall performance of this technology, however, is still inconsistent. • Further improvement in the technology and larger multicenter studies are needed to propel electromagnetic guidance to the forefront of the diagnostic and therapeutic algorithm for solitary pulmonary nodules.
Advantages • Reach and sampling of peripheral lung lesions • Taking tissue sample • Histopathologic diagnosis opportunity • Less thoracotomy - surgery • Not need general anesthesia • No radioactivity risk
Disadvantages • Cost of SD system • Add approx. 400 USD cost for locatable guide that is used each one for every patient. • Cost of bronchoscopy procedure • In Turkey, approx. 100 USD • Experiment need • Risk of pneumothorax • Lack of data (RCT)