Download
1 / 60
1.55k likes | 5.72k Views
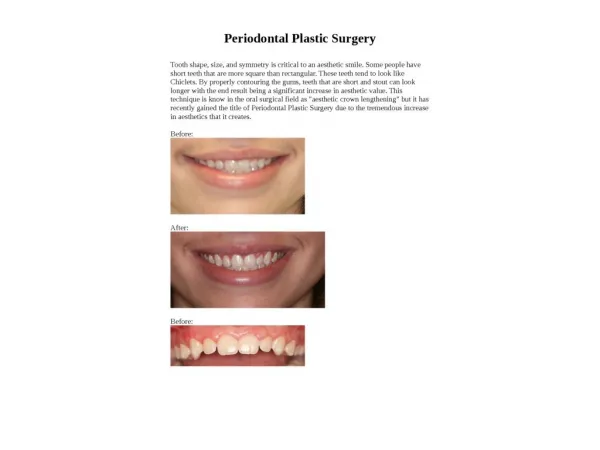
Periodontal Flap Surgery. Purpose. To gain access to deeper periodontal structures with direct vision . Relocation of the frenulum Maintenance of the attached tissue Pocket elimination and regeneration. Indications. Pockets > 5mm persisting after phase I therapy

E N D
Purpose To gain access to deeper periodontal structures with direct vision. Relocation of the frenulum Maintenance of the attached tissue Pocket elimination and regeneration
Indications • Pockets > 5mm persisting after phase I therapy • Bony pockets and interdentalcraters • Bony lesions in the furcations • Need for surgical crown lengthening • When to open up a flap? complicated morphology like: • Deep and narrow pocket • Difficult to achieve the correct angle
Contraindications • Shallow, supraalveolar pockets • subgingival scaling/rootplaning • Esthetically sensitive areas • Fibrous thickened gingiva • gingivectomy more favorable morphology
Instruments Small elevators for mobilization of the mucoperiosteal flap
Principles of Flap Design • Local flap • outlined by a surgical incision • carries its own blood supply • allows surgical access to underlying tissues • can be replaced in the original position • can be maintained with sutures and is expected to heal • Used in oral surgical, periodontic, and endodontic procedures to gain access.
Principles of Flap Design • Complications • Flap necrosis • Flap Dehiscence • Flap Tearing • Injury to Local Structures
A. Flap necrosis Principles of Flap Design • Base > Free margin • to preserve an adequate blood supply • unless a major artery is present in the base • Width of Base > Length of Flap*2 • less critical in oral cavity, but length < width • a long, straight incision with adequate flap reflection heals more rapidly than a short, torn incision. • An axial blood supplyin the base • Hold the flap with a retractor resting on intact bone to prevent tension.
B. Flap Dehiscence Principles of Flap Design • The incisions must be made over intact bone • If the pathologic condition has eroded the buccocortical plate, the incision must be at least 6 or 8 mm away from it. • The incision is 6 to 8 mm away from the bony defect created by surgery. • Gently handle the flap's edges • Do not place the flap under tension • Do not cross bony prominences, ex: canine eminence
B. Flap Dehiscence Principles of Flap Design
C. Flap Tearing Principles of Flap Design • Envelope flaps • an incision around the necks of several teeth. • extends 2 teeth anterior and 1 tooth posterior. • If not provide sufficient access… • Vertical (oblique) releasing incisions: • extends 1 tooth anterior and 1 tooth posterior. • started at the line angle of a tooth. • carried obliquely apically into the unattached gingiva. • If cross the papilla localized periodontal problems
D. Injury to Local Structures Principles of Flap Design • Mandible: lingual n. & mental n.
D. Injury to Local Structures Principles of Flap Design • Maxilla: greater palatine a. & nasopalatine n./a.
Basic Incisions • Can be sulcular, crestal, or inverse bevel
Full thickness (mucoperiosteal) Basic Incisions a: sulcular b: crestal Depending on the amount of attached tissue present
Basic Incisions Split/partial thickness (mucosal) In areas of thin bony plates and for mucogingival procedures
Basic Incisions 2. inversebeveled incision to the crest of bone. Modified flap (mucoperiosteal) 1. gingivectomy Incision for pocket reduction Requires adequate attached keratinized gingiva On the palate, enlarged tissue, or with limited access
Types of Mucoperiosteal Flaps Envelope/sulcular incision Envelope with one releasing incision (three-corner flap) Envelope with two releasing incisions (four-corner flap) Full-thickness mucoperiostealflap
1. Envelope/Sulcular flap 2 teeth anterior 1 tooth posterior Types of Mucoperiosteal Flaps
2. Three-corner flap 1 tooth anterior 1 tooth posterior Types of Mucoperiosteal Flaps • Greater access in an apical direction, especially in the posterior aspect of the mouth
3. Four-corner flap 1 tooth anterior 1 tooth posterior Types of Mucoperiosteal Flaps • rarely indicated
1 Inverse bevel incision 0.5~2mm, extending to the alveolar crest. Thins gingival tissue and permits compete closure of the interdental osseous defects postoperatively.
1 Flap reflection. Full thickness mucoperiosteal flap is reflected to permits visualization.
1 Crevicular incision between the hard tooth and the diseased pocket epi., to the depth of the junctional epi.
1 Horizontal incision carried along the alveolar crest
1 Root planing with direct vision
1 Complete coverage of interdental defects
2 Sulcularly, crestally, or full-thickness flap labially positioned inverse beveled incision to bone Flap completed, reflected off bone Flap is apically positioned and sutured
2 A: The internal bevelled, scalloped incision is used for pocket elimination through apical repositioning of the flap. B: The flap positioned apically for pocket elimination.
Crestal incision with blade, partial-thickness flap parallel to long axis of tooth Flap raised by sharp dissection, periosteum retained over bone Flap is apically positioned at or below alveolar crest
No alveolar mucosa is present on the palate to permit apical positioning. Pocket elimination by palatal flap that just covers the contours of the bone to eliminate osseous defects. Requires skill and experience.
Osteoplasty Osseous grooving, peprmits better adaption of flaps to facilitate plaque removal alter healing