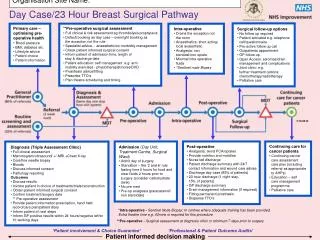
Surgical Prophylaxis and Infection Rates Analysis
340 likes | 389 Views
Understanding surgical prophylaxis and infection rates in different types of surgeries. Importance of antibiotic timing for prevention. Analysis of site-specific infection rates. Recommended antibiotics for various surgeries.

Surgical Prophylaxis and Infection Rates Analysis
E N D
Presentation Transcript
Surgical prophylaxis 衛生福利部 疾病管制署 中區傳染病防治醫療網 王任賢 指揮官
預防性投藥 對完全沒有疾病的人投予藥物 接受藥物的人必須在經歷某種介入措施後會有超過10%的感染率才有投予的價值
Classification of surgical wounds • Clean • Clean-contaminated • Contaminated • Dirty
Surgical wound infection rates • Clean wound 1-2% • Clean prosthetic < 5% • Clean contaminated < 10% • Contaminated appendix < 10% large bowel 15-20% dirty fecal peritonitis > 60% Am J Surg 1994;167:15S-19S
可以考慮不投予預防性抗生素之手術名稱 疝氣修補手術 甲狀腺切除手術 淋巴切除手術 白內障切除手術 子宮肌瘤切除術 -------------
Site-specific infection rates without antimicrobial coverage Site of operation Wound infection rate (%) Colorectal 40 Appendix, normal/inflamed/gangrenous 14/16/56 Gastroduodenal, not specified 27 Duodenal ulcer, elective/obstructed/perforated 5/16/18 Gastric ulcer 23 Gastric tumor 31 UGI bleeding 49 Cholecystectomy 15 Vascular 13 Head and neck 45 Annu Rev Med 1993;44:385-93
Definition of prophylaxis vs therapy • Prophylaxis antimicrobials given prior to attachment of contaminating bacteria to host tissues at the operation site • Therapy antimicrobials given after possible attachment
“the routine use of prophylaxis in clean operations is unnecessary and undesirable” Dr. Maxwell Finland RI Med J 1960;43:499-504
Kinetics of bacterial growth after its seeding into a surgical wound: I Surgical Procedure
Kinetics of bacterial growth after its seeding into a surgical wound: II Surgical Procedure serum hematoma Antibiotics
Kinetics of bacterial growth after its seeding into a surgical wound: III Surgical Procedure Antibiotics in clot Antibiotics in serum Antibiotics administrated
Timing of penicillin injection and the size of staphylococcal lesion in guinea pig Staphylococcal lesions Staphylococcal lesions + PC Mean 24 hr lesion size (mm) Killed staphylococcal lesions Lesion age in hrs when penicillin injected Surgery 1961;1:161-8
Timing of prophylactic antibiotics and rates of surgical-wound infection Time of No. of No. (%) of Relative risk Odds ratio Administration patients infection (95% CI) Early 369 14 (3.8) 6.7 (2.9-14.7) 4.3 Preoperative 1708 10 (0.59) 1.0 Perioperative 282 4 (1.4) 2.4 (0.9-7.9) 2.1 Postoperative 488 16 (3.3) 5.8 (2.6-12.3) 5.8 All 2847 44 (1.5) Early: 2-24 hrs before incision Preoperative: 0-2 hrs before incision Perioperative: within 3 hrs after incision Postoperative: > 3 hrs after incision NEJM 1992;326:281-6
Rates of surgical-wound infection vs timing of prophylaxis Infection rate (%) Hours after incision NEJM 1992;326:281-6 Incision
Wound infection related to time of initiation of prophylaxis with cefazolin Area of % infection when antibiotic was begun operation 8-12 hr 1 hr 1-4 hr Not given preop preop postop Gastric 5 4 17 22 Biliary 3 < 3 9 11 Colonic 6 6 15 15 Ann Surg 1976;184:443
Antibiotic levels in serum/0.4% fibrin clot in relation to MIC for E. coli & B. fragilis Antibiotics Min after IM MIC (mg/L) 30 60 240 EC BF Gentamicin (S) 14.3 16.5 4.1 4 -12.5 mg/kg (C) 0.6 0.7 < 2 Ampicillin (S) 65.0 8.0 4.4 16 -200 mg/kg (C) 2.0 < 2 < 2 Cefoxitin (S) 360 150 3.6 8 16 375 mg/kg (C) 4.2 20 < 4 Clindamycin (S) 25.0 60.0 18.0 - 0.2 100 mg/kg (C) < 0.1 < 0.1 < 0.1 - 0.2 Arch Surg 1986;121:163-8
Objectives of prophylaxis & therapy • Clean surgery prevent extrinsic contamination of prosthesis • Clean-contaminated surgery reduce the number of mucosa-associated colonizing bacteria • Contaminated surgery (therapy) eradicate bacteria that have already become attached to host tissues
Infection rates in clean neurosurgical operations, controlled studies Infection rate (%) with without relative prophylaxis prophylaxis risk 1984 Geraghty 0.5 3.6 7.4 1986 Mollman NA NA 5.6 1986 Shapiro 2.8 11.7 4.1 1987 Young 1.0 3.8 3.9 1988 Blomstedt 1.8 7.4 4.1 Neurosurgery 1989;24:401-5
Differing actions of antimicrobials in therapy and prophylaxis • Rheumatic fever oral sulfonamides, oral penicillins • Postpartum endometritis after C/S cefazolin, cefoxitin, cefotetan • Surgical prophylaxis 2nd, 3rd cephalosporin, cefazolin
Recommended antibiotic for prophylaxis • Gynecologic surgery C/S cefazolin (1g IV) after cord clamp Hysterectomy cefazolin (1g IV) Abortion cefazolin (1g IV) • Orthopedic surgery Open reduction cefazolin (1g IV) Internal fixation cefazolin (1g IV) Joint replacement cefazolin (1g IV) Spinal fusion No proven benefit Leg amputation cefoxitin (2g IV)
Recommended antibiotic for prophylaxis • General surgery Gastric resection cefazolin (1g IV) Gastrostomy cefazolin (1g IV) Biliary surgery cefazolin (1g IV) Colon surgery oral prophylaxis or cefoxitin, cefotetan (2g IV) Appendectomy cefoxitin, cefotetan (2g IV) Hernia repair cefazolin (1g IV)
Levels of cefazolin & cephalothin in serum and bone tissue after IV dose of 1 gm mg/g Surg Gyn Obstet 1989;168:283-9 min
Results of cephalosporin prophylaxis for experimental wound in mice Contaminant Treatment No. Mean CFU/g Infection rate (%) S. aureus cefazolin 42 22.5K 2.4 S. aureus cefamandole 42 40.8K 7.1 S. aureus cefotaxime 42 29.0K 2.4 S. aureus saline 42 17.9K 76.2 E. coli cefazolin 42 6.8K 0 E. coli cefamandole 42 10.9K 0 E. coli cefotaxime 42 90.1K 2.4 E. coli saline 42 25.7K 66.7 Fecal cefazolin 41 54.1K 9.8 Fecal cefamandole 41 36.6K 4.9 Fecal cefotaxime 41 40.5K 9.8 Fecal saline 41 20.9K 85.4 Surgery 1985;98:30-4
Comparative trial of cefazolin and moxalactam for prophylaxis of abdominal hysterectomy: total infection morbidity Cefazolin Moxalactam Two-sided (N=108) (N=100) p value Serious infection 1 (1%) 4 (4%) NS Minor wound 5 (5%) 2 (2%) NS UTI 5 (5%) 15 (15%) 0.021 Febrile morbidity 25 (23%) 17 (17%) NS Total 36 (34%) 38 (38%) NS Obstet Gynecol 1985;66:372-6
Intraoperative concentration (mg/ml) of the cephalosporins Specimen Cefamandole Cefoxitin Cefazolin Serum At drug infusion 119.7 96.3 140.8 At 0.25 h 98.6 79.4 130.9 At 1 h 56.1 45.7 105.9 At 2.2 h 23.8 20.3 76.4 At 4 h 7.3 6.9 43.7 Hematoma 21.1 17.2 41.9 Muscle 14.7 12.6 15.7 J Bone Joint Surg Am 1985;67:921-4
Prophylactic antibiotics in appendicitis Prophylactic antimicrobial No. of patients Infection operated rate (%) Placebo 3951 21.7 Cephalosporins 336 15.8 Metronidazole 1325 10.8 Broad-spectrum penicillins 114 8.8 Antiaerobe/anaerobe 261 2.7 Infect Dis Clin N Am 1992;6:613-25
外科預防性投藥常碰到的疑惑 • 已經在接受抗生素治療時,還該給嗎? • 外科預防性投藥等同於心內膜炎的預防性投藥嗎? • 在一個複雜的手術後,抗生素需一直給到所有管子均拔除為止嗎? • 在作心導管、PTCA、或放心律調節器時該routine給預防性投藥嗎?
Impact of Prolonged Surgical Prophylaxis • DESIGN: Prospective • POPULATION: CABG patients (N=2641) Group 1: pts who received < 48 hours of AP Group 2: pts who received > 48 hrs of AP
Impact of Prolonged Surgical AP • OUTCOMES • Incidence of SSI • Isolation of a resistant pathogen • RESULTS: 43% of patients received AP > 48 hr SSIIncidence • <48 hrs group: 8.7% (131/1502) vs • >48 hrs group: 8.8% (100/1139), p=1.0 Antimicrobial resistant pathogen • OR 1.6 (95% CI 1.1-2.6)
Special considerations : I • Reoperation through fresh or healing clean wound • Elective large bowel operation clear liquid diet + whole gut lavage 1 g neomycin + erythromycin 1 pm, 2 pm, 11pm the day before operation • Percutaneous endscopic gastrostmy • Cardiac operations with cardiopulmonary bypass
Special considerations : II • Cesarean sections low risk vs high risk • Vascular graft, vascular reconstructions, and vascular-access shunts • Penile prostheses, LN dssections, & VP shunts • Early treatment of compound fractures & abdminal trauma
Special considerations : III • Prevention of septic arthritis in a preexisting orthopedic prosthesis • Replacement of prostheses and need for culture • Blood loss during operation • Prolonged operation time