Download
1 / 33
340 likes | 712 Views
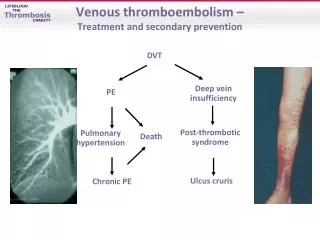
Venous Thromboembolism in the Surgical Patient: Prophylaxis and Treatment. Pamela Hebbard August 11, 2005. Prophylaxis . Scenario 1. You are going through consent with a 60 y.o. F going for laparotomy for non-resolving SBO.

E N D
Venous Thromboembolism in the Surgical Patient:Prophylaxis and Treatment Pamela Hebbard August 11, 2005
Scenario 1 • You are going through consent with a 60 y.o. F going for laparotomy for non-resolving SBO. • What is the risk of VTE in the average general surgery patient without prophylaxis? • A. 10% DVT, 0.001% fatal PE • B. 5% DVT, 0.01% fatal PE • C. 25% DVT, 0.05% fatal PE • D. 50% DVT, 1% fatal PE
Incidence • In general surgery patients without prophylaxis: • 15 - 30% DVT • 0.2% - 0.9% fatal PE • Risk is higher with pelvic surgery, cancer surgery • Of all surgery orthopedic surgery carries the highest risk, at 50-60% DVT
Scenario 2 • 52 y.o. F going for R hemicolectomy for cecal cancer. What will you choose for VTE prophylaxis? • A. aspirin to start post-op • B. a low-dose heparin • C. mechanical compression device/stockings • D. warfarin to start post-op • E. some combination of the above
Methods of Prophylaxis • 1. Aspirin • 20% risk reduction compared to placebo (5 trials) • 2. Graded compression stockings • 44% risk reduction • Knee-length equally effective and easier to use than thigh-length • Need to be fitted for them
Methods of Prophylaxis • 3. Heparins • Low-molecular weight and unfractionated • ~70% risk reduction • Equally effective • Risk of bleeding related to dose (LMWH)
Methods of Prophylaxis • 4. Intermittent pneumatic compression • 88% risk reduction • equally effective as heparin • Probably better than stockings • From small, older studies • Also need to be fitted and requires equipment
Methods of Prophylaxis • 5. Warfarin • does have a risk reduction • Older studies, mostly orthopedics • Impractical • 6. Heparin + mechanical method • Stockings + LDUH have been shown to enhance protection from VTE by a further 75% (from 15% to 4%).
Scenario 3 • You have chosen to use a heparin as VTE prophylaxis for your post-op patient with cecal ca. Exactly what order will you write? • A. heparin 5000 u sc bid • B. heparin 5000 u sc tid • C. heparin 15000 u sc bid • D. heparin ACS/DVT protocol • E. enoxaparin 30mg sc bid • F. enoxaparin 40 mg sc od • G. enoxaparin 80 mg sc bid (1 mg/kg) • H. enoxaparin 120 mg sc od (1.5 mg/kg)
Heparin Dosing-Prophylaxis • Unfractionated heparin: • 5000 u bid/tid • Lovenox: • 30 mg sc bid • 40 mg sc od**
Scenario 4 • Patient 1: 20 y.o. M - inguinal hernia repair • Patient 2: 60 y.o. M - APR • What post-op orders will you write? • A. no heparin for either • B. heparin for both • C.1 - none, 2 - heparin • D.1 - heparin bid, 2 - heparin tid
Risk Stratification • Low - Risk • “Minor” surgery • <40 y.o • No additional risk factors • Recommendation • Early ambulation only
Risk Stratification • Moderate Risk • Minor surgery in patients with additional risk factors • Any surgery in pts aged 40-60 w/o additional risk factors • Major surgery in patients <40 y.o w/o additional risk factors • Recommendation • Heparin 5000 bid • LMWH <= 3400 IU/day (Lovenox 30mg od) • May consider stockings if contraindication to heparin
Risk Stratification • High Risk • Multiple risk factors • age > 60 y.o. • Age 40-60 y.o. with an additional risk • Recommendation • Heparin 5000 tid • LMWH >3400 IU/day (Lovenox 40mg od or more)
Risk Stratification • Very High Risk • Major surgery in >40 y.o. with: cancer, previous VTE, or known hypercoagulable state • Major ortho surgery, elective neurosurgery, multiple trauma, acute SCI • Recommendation • High risk heparin dosing + stockings/ IPC
Scenario 5 • You are going to give your pt heparin prophylaxis for major abdominal surgery. When do you give the first does? • A. 2 hrs pre-op • B. in recovery room • C. once up to the floor • D. after the epidural comes out
Timing • Optimal timing is 2 hrs pre-op • DVT’s begin intra-operatively • Timing may need to be adjusted if neuraxial anesthesia is being used (no strict guidelines?)
Scenario 6 • Consider again your patient with colon cancer. How long should you continue her VTE prophylaxis? • A. until ambulating • B. 7 days • C. until discharge • D. 4 weeks • E. 6 months
Timing • For most patients, heparin until ambulating well is satisfactory. • For high risk patients, heparin should continue for 7-10 days minimum • Abdominal or pelvic surgery for cancer: 4 weeks of LMWH reduces the incidence of DVT compared to 1 week.
Scenario 7 • Your post-op patient is noted to have a swollen firm left calf. U/S documents proximal DVT. What is your initial treatment? • A. heparin 5000 u sc tid • B. heparin ACS/DVT protocol • C. enoxaparin 30mg sc bid • D. enoxaparin 80 mg sc bid (1 mg/kg) • E. enoxaparin 120 mg sc od (1.5 mg/kg)
Initial Treatment • Choice of heparin infusion or LMWH sc • Both shown to be equally effective and safe • Same treatment for DVT and PE • LMWH easier to administer, cheaper--assuming no contraindications
Initial Treatment • Start warfarin at same time as heparin • Continue heparin for at least 5 days and INR 2-3 • Out-patient therapy is equally as safe as in-hospital treatment
Scenario 8 • 70 y.o. M post-op from Hartmann’s for diverticulitis. DVT post-op. PHx DM, HTN, CAD, and stroke. How long does he continue on warfarin? • A. 3 mo at INR 2-3 • B. 6 mo at INR 2-3 • C. 12 mo at INR 2-3 • D. 6 mo at INR 2-3, then indefinitely at INR 1.5-2 • E. Indefinitely at INR 2-3
Warfarin Therapy • First episode of DVT -- usually 6 months • DVT due to transient risk factor (Surgery): 3 months of tx may be considered • PREVENT and ELATE have shown that indefinite treatment does decrease the risk of recurrence. They disagree on the necessary target INR. • Long-term therapy needs to be balanced against the risk of bleeding.
Scenario 9 • 62 yo w/ recently diagnosed mucinous adenocarcinoma in the liver with no known primary. Presents with syncope, now normotensive, and found to have PE on CT. Treatment? • A. Start LMWH and warfarin, continue warfarin indefinitely or until cure • B. Start heparin drip and warfarin, continue warfarin indefinitely. • C. LMWH indefinitely • D. LMWH for 6 months
VTE in Cancer Patients • LMWH is better than unfractionated heparin for cancer patients. • Antithrombotic and antineoplastic effects • LMWH is better than warfarin for long-term tx in cancer patients (less fatal bleeding)
Scenario 10 • You are called to see a post-op pt with a swollen leg. It is indeed swollen, tense and a deep red-purple colour. You note some skin necrosis. An U/S documents DVT. Treatment? • A. IV heparin • B. full-dose Lovenox • C. debride skin • D. thrombectomy
Surgery for DVT • Phlegmasia ceruluea dolens/ venous gangrene is an absolute indication for surgery. • Femoral venotomy • Interventional radiology • High incidence of post-phlebitic syndrome
Other Treatments • Thrombolytics • Controversial • Best evidence in unstable patient with PE • Indicated in massive ileofemoral thrombolysis and low-risk to bleed • New medications • Fondaparinux • ximelagatran
IVC Filters • Protect against fatal PE • In general, for use in patients with contraindication to anticoagulation • May consider filter + anticoag is patient with severe cardiopulmonary dz where recurrent PE may be fatal. • Information based on poor, older studies • Retrievable filters (new)
Further Info • ACCP Guidelines Chest, Sept 2004, Vol126, supp 3. • AJS 2005, 189:14-25.