Download
1 / 36
420 likes | 1.05k Views
Vitamin D metabolism. Dr Salah Mansy Consultant Paediatrician Conquest Hospital. Objectives. Understand physiology and pathophysiology of vitamin D Clinical presentations of vit D deficiency/insufficiency Prevention and treatment of vit D deficiency/insufficiency Thoughts for the future.

E N D
Vitamin D metabolism Dr Salah Mansy Consultant Paediatrician Conquest Hospital
Objectives • Understand physiology and pathophysiology of vitamin D • Clinical presentations of vit D deficiency/insufficiency • Prevention and treatment of vit D deficiency/insufficiency • Thoughts for the future
Human skeleton • Protein matrix: osteoid (90%), osteocalcin and other proteins • calcium phosphate, calcium carbonate, sodium, magnesium, and citrate • Dynamic
Definitions • Rickets: only in growing children. Poor mineralisation before fusion of the epiphyses. • Osteomalacia: poor mineralization at all ages. • All patients with rickets have osteomalacia, but not all patients with osteomalacia have rickets • Osteoporosis: poor mineralization and loss of bone volume
Epidemiology • A disease of 19th and 20th century in northern Europe and the United States • Resurgence of vitamin D deficiency in UK • Recent prevalence data in UK children is lacking • Adult study • 46.6% of white adults are vit D deficient. Am J Clin Nutr 2007;85:860-8 • One in 8 white, 1 in 4 African Caribbean, 1 in 3 Asian adults are vit D deficient. Ann Clin Biochem 2006; 43:468-73
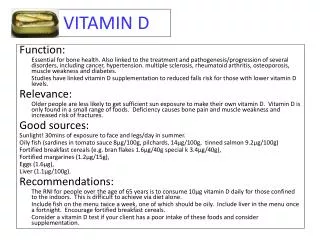
Risk factors • Exclusively breast fed • Multiple short interval pregnancies • Vegetarian (or other non-fish eating) diet • Lack of sunlight exposure • Cultural influence on dress • Sedentary indoors lifestyle • Sunscreen use • Fear of cancer • Pigmented skin • Obesity • Malabsorption, short bowl or cholestatic liver disease • Use of anticonvulsants, rifampicin, cholestyramin, glucocorticoids or highly active antiretroviral treatment (HAART)
Sources • Ultraviolet B sunlight exposure 90% of supply • Oily fish • Cod liver oils • Infant formula milk (400 IU/L) • some breakfast cereals, breads and margarine • Breast milk: low (12–60 IU/L) • Egg yolk (20 IU) • Mushrooms (small quantities)
Table 2: Recommended Dietary Allowances (RDAs) for Vitamin D [1] * Adequate Intake (AI)
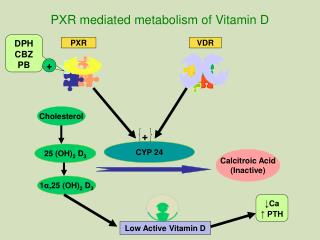
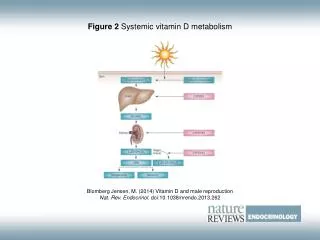
The metabolic pathway of vitamin D, indicating its conversion to the hormone 1,25(OH)2D3 and to 24,25(OH)2D3. Vitamin D2 (ergosterol), of plant origin, appears to undergo similar metabolic steps.
Physiology • 1,25-D: • Intestine: marked increase in calcium absorption, less significant increase in phosphorus absorption ( most dietary phosphorus absorption is vitamin D–independent) • Bone resorption • PTH secretion suppression (negative feedback loop) • Kidney: inhibits its own synthesis and increases the synthesis of inactive metabolites • 25-D is the standard method for determining a patient's vitamin D status because there is little regulation of the liver hydroxylation step.
Physiology • Parathyroid hormone (PTH) and vitamin D are the principal regulators of calcium homeostasis • Calcitonin and PTH-related peptide (PTHrP) are important primarily in the fetus. • Phosphate homeostasis is regulated by the kidneys because intestinal phosphate absorption is nearly complete and renal excretion determines the serum level
Causes of Rickets • Vitamin D deficiency • Nutritional vitamin D deficiency • Congenital vitamin D deficiency • Secondary vitamin D deficiency • Malabsorption • Increased degradation • Decreased liver 25-hydroxylase • Vitamin D–dependent rickets type 1 • Vitamin D–dependent rickets type 2 • Chronic renal failure • Calcium deficiency • Intake • Absorption • Rickets of prematurity • Phosphate deficiency • Intake • Absorption • Renal diseases • Renal tubular acidosis • Rickets of prematurity
Diagnosis: History • History of poor growth, delayed walking, waddling gait, dental caries, pneumonia, and hypocalcaemia symptoms • Decrease dietary intake • Decrease skin synthesis: clothing, skin pigmentation, sun screen, season • Malabsorption due to liver or intestinal disease • Renal disease • Drugs e.g. Phenobarbital, phenytoin, aluminium-containing antacids, rifampicin, cholestyramin, glucocorticoids or highly active antiretroviral treatment (HAART) • Maternal risk factors for nutritional vitamin D deficiency • Family history of genetic disorders, leg deformities, difficulties with walking, or unexplained short stature , unexplained sibling death (Cystinosis)
Clinical features: General • Failure to thrive • Listlessness • Protruding abdomen • Muscle weakness (especially proximal) • Fractures
Clinical features: Head • Craniotabes • Frontal bossing • Delayed fontanelle closure • Delayed dentition; caries • Alopecia (vitamin D–dependent rickets type 2)
Clinical features: Chest • Rachitic rosary • Harrison groove • Respiratory infections and atelectasis
Clinical features: Extremities • Leg pain • Enlargement of wrists and ankles • Valgus or varus deformities • Coxa vara • Anterior bowing of the tibia and femur • Windswept deformity (combination of valgus deformity of 1 leg with varus deformity of the other leg)
Clinical features: Back • Scoliosis • Kyphosis • Lordosis
Clinical features: Hypocalcaemia symptoms • Tetany • Stridor due to laryngeal spasm • Seizures Stebbing C, Mansy S, Kanabar D (2002) The first reported presentation of rickets with metabolic seizures. Hospital Medicine 63: 690-691
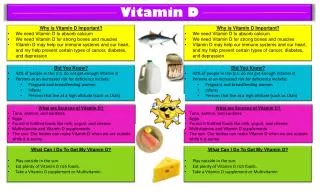
(A) a normal child (B) a child with rickets: metaphyseal fraying and cupping of the distal radius and ulna.
X-rays of the knees in a 7 yr old girl with distal renal tubular acidosis and rickets. A, At initial presentation, there is widening of the growth plate and metaphyseal fraying. B, Dramatic improvement after 4 mo of therapy with alkali.
a two-year old rickets sufferer, with a marked genu varum, (bowing of the femurs) and decreased bone opacity, suggesting poor bone mineralization
VDDR: vitamin D–dependent rickets XLH: X-linked hypophosphatemic rickets ADHR: autosomal dominant hypophosphatemic rickets HHRH: hereditary hypophosphatemic rickets with hypercalicuria Pi: phosphorus RD: relatively decreased (because it should be increased given the concurrent hypophosphatemia
Consequences of untreated vitamin D deficiency • Skeletal complications • Musculoskeletal pain particularly in adolescence. Arch Dis Child 2011;96:694-6 • Reduced whole body bone mineral content and bone mass even at 9 years of age. Lancet 2006; 367:36-43 • Hypertension, hyperglycaemia and metabolic syndrome in adolescents. Pediatrics 2009 Aug 3 • Type 1 diabetes, multiple sclerosis, malignancy and schizophrenia. Pediatrics 2008;122:398-417 • Cardiomyopathy (3 deaths in the last 10 years in UK). Heart 2008;94:581-4
Threshold for intervention for vit D deficiency 25-hydroxyvitamin D level reliably determine vit D status. Nutr Rev 2008;66:S153-64 <25 nmol/l = severe deficiency = treat 25-50 nmol/l = insufficiency = supplementation 51-75 nmol/l = sufficiency = lifestyle advice >250 nmol/l = excess = stop treatment Arch Dis Child 2011,96:614-615
Prevention of vit D deficiency in UK • Huge economic burden and preventive strategies are cost effective. Prog Biophys Mol Biol 2009;99:104-13 • Healthy Start scheme 2006. http://www.healthystart.nhs.uk • Free vit D to economically disadvantaged children and young mothers • Restrictive qualification criterion for supplements • Only children under 4 • Only mothers with a very limited income • Asylum seekers are not entitled • Inconsistent dissemination of message regarding supplementation to pregnant women • Poor availability of supplements
Prevention of vit D deficiency in UK • Recommendations for vit D supplementation have not generally been implemented. Update on Vitamin D. Position Statement by the Scientific Advisory Committee on Nutrician. 2007. http://www.sacn.gov.uk • Better targeting of health resources to antenatal care, pregnant mothers and at risk children • Extending the range of food fortified with vit D • Clarification of the risk associated with UV radiation against the risk of deficient vit D synthesis
Vit D preparations • Ergocalciferol (yeast derived D2) • Oily solution 3000 IU/ ml • Tablets 10 000 IU or 50 000 IU • Tablets calcium 400 mg and vitamin D 400 IU • Parenteral 300 000 IU/ ml • Colecalciferol (fish or lanoline derived D3) • Dalvit 400 IU/ 0.6 ml • Abidec 400 IU / 0.6ml • Healthy Start vitamin drops 300 IU/ 5drops • Tablets 20 000 IU • Alfacalcidol (one Alpha Hydroxycolecalciferol) • Oral/IV in persistent cases, renal, cholestatic liver disease
Treatment of deficiency • < 6months: 3000 IU daily for 8-12 weeks • > 6 months: 6000 IU daily for 8-12 weeks • > 1 year: 300,000–600,000 IU orally or intramuscularly as 2–4 doses over 1 day • Adequate dietary calcium and phosphorus • Daily vitamin D intake of 400 IU/day
Treatment of insufficiency • < 6 months: 200-400 IU daily • > 6 months 400-800 IU daily
Unanswered questions • Would eradication of vitamin D insufficiency in the UK reduce cancer incidence and improve cancer outcome? • Does poor vitamin D status cause obesity, or is it a consequence of obesity? • Are individuals genetically susceptible to vitamin D insufficiency or toxicity? • How much does vitamin D insufficiency contributes to north/south health inequalities?
Summary points • Vitamin D insufficiency is common in UK • Vitamin D deficiency presentation is different in different age group • Vitamin D deficiency is easy to treat • Vitamin D is linked to other health problems e.g. cardiovascular, DM type 2 etc. • Vitamin D insufficiency is preventable however robust measures are not yet in place