Download
1 / 70
860 likes | 1.14k Views
Discover the impact of statin therapy on reducing cardiovascular events in diabetic and nondiabetic patients. Learn about the importance of LDL-C reduction and the risks associated with low HDL-C and elevated TG levels.

E N D
Beyond LDL-C Christie M. Ballantyne, MD Professor, Department of Medicine Chief, Section of Atherosclerosis and Vascular Medicine Director, Center for Cardiovascular Disease Prevention Baylor College of Medicine Methodist DeBakey Heart Center Houston, Texas
Statin Therapy Reduces Clinical Events in Patients With and Without Diabetes Meta-Analysis of 14 Statin Trialsa All-Cause Mortality Major Vascular Eventsb 21% Reduction P<.0001 Control Treatmentc 21% Reduction P<.0001 9% Reduction P=.02 13% Reduction P<.0001 Events, % Diabetes No Diabetes Diabetes No Diabetes a4.3-year mean follow-up of 18 686 patients with diabetes; n = 71 370 patients with no diabetes bNonfatal MI, CHD death, stroke, or coronary revascularization cEvent rate per 1 mmol/L (39 mg/dL) reduction in LDL-C CTT Collaborators. Lancet. 2008;371:117-125.
Statin Therapy Reduces Major Vascular Events in Patients With and Without Prior Vascular DiseaseaCTT Meta-Analysis of 14 Statin Trialsb 20% Reduction Control Treatmentd 21% Reduction 27% Reduction Major Vascular Eventsc, % 22% Reduction Diabetes No Diabetes Diabetes No Diabetes With Prior Vascular Diseasea No Prior Vascular Diseasea aCHD, cerebrovascular disease, or peripheral arterial diseaseb4.3-year mean follow-up of 18 686 patients with diabetes; n = 71 370 patients with no diabetes cNonfatal MI, CHD death, stroke, or coronary revascularization dEvent rate per 1 mmol/L (39 mg/dL) reduction in LDL-C CTT Collaborators. Lancet. 2008;360:117-125.
CHD events occur in patients treated with statins 19.4 12.3 10.2 8.7 6.8 5.5 Residual Cardiovascular Risk in Major Statin Trials 28.0 Placebo Statin Patients Experiencing Major CHD Events, % 15.9 13.2 11.8 10.9 7.9 4S1 LIPID2 CARE3 HPS4 WOSCOPS5 AFCAPS/ TexCAPS6 N 4444 9014 4159 20 536 6595 6605 LDL -35% -25% -28% -29% -26% -25% Secondary High Risk Primary 14S Group. Lancet. 1994;344:1383-1389. 2LIPID Study Group. N Engl J Med. 1998;339:1349-1357. 3Sacks FM, et al. N Engl J Med. 1996;335:1001-1009. 4HPS Collaborative Group. Lancet. 2002;360:7-22. 5Shepherd J, et al. N Engl J Med. 1995;333:1301-1307. 6 Downs JR, et al. JAMA. 1998;279:1615-1622.
Statistically significant, but clinically inadequate CVD reduction1 Residual CVD Risk in Patients Treated With Intensive Statin Therapy Standard statin therapy Intensive high-dose statin therapy Patients Experiencing Major CVD Events, % PROVE IT-TIMI 222 IDEAL3 TNT4 N 4162 8888 10 001 LDL-C,a mg/dL 95 62 104 81 101 77 1Superko HR. Br J Cardiol. 2006;13:131-136. 2Cannon CP, et al. N Engl J Med. 2004;350:1495-1504. 3Pedersen TR, et al. JAMA. 2005;294:2437-2445. 4LaRosa JC, et al. N Engl J Med. 2005;352:1425-1435. aMean or median LDL-C after treatment
Residual Risk Residual Risk Residual CVD Risk Is Particularly High in Patients With Diabetes Treated With Statins Meta-Analysis of CHD Patients in 14 Statin Trialsa Control CVD Risk Higher Than Patients With No Diabetes on Placebo Treatmentc Major Vascular Event Rateb, % Diabetes No Diabetes a4.3-year mean follow-up of 18 686 patients with diabetes; n = 71 370 patients with no diabetes bNonfatal MI, CHD death, stroke, or coronary revascularization cEvent rate per 1 mmol/L (39 mg/dL) reduction in LDL-C CTT Collaborators. Lancet. 2008;371:117-125.
250 200 177 219 180 Controls Controls 200 160 CHD CHD 141 139 138 140 152 120 150 134 100 Plasma Lipid Concentration, mg/dL Plasma Lipid Concentration, mg/dL 110 80 100 60 57 45 47 35 40 50 20 0 0 LDL-C TG HDL-C LDL-C TG HDL-C Elevated Triglycerides and Low HDL-C in Patients With Premature CHD Men Women † * † * *P<.005 as compared with controls †P<.05 as compared with controls Genest JJ Jr, et al. Circulation. 1992;85:2025-2033.
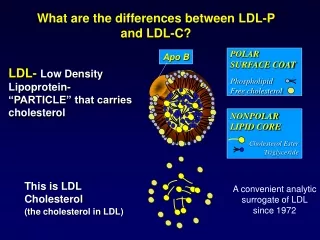
Atherogenic Dyslipidemia in Patients With Diabetes and the Metabolic Syndrome • High triglyceride levels • TG-rich remnant lipoproteins (VLDL) • Altered metabolism of LDL and HDL particles • While LDL-C may not be increased, LDL particle number may be significantly increased • Predominantly small, dense LDL particles • Low levels of HDL-C(may reduce RCT) Haffner SM. Diabetes Care. 2003;26(suppl 1):S83-S86. Garvey WT, et al. Diabetes. 2003;52:453-462.
NCEP ATP III: HDL-C Is an Independent Risk Factor for CHD • A low HDL-C level is strongly and inversely associated with CHD risk • Independent relationship holds after correction for other risk variables in multivariate analysis • A low HDL-C level often correlates with elevations of serum triglycerides and remnant lipoproteins • Mechanisms by which HDL may be antiatherogenic • Promotion of reverse cholesterol transport (RCT) • Antioxidant and anti-inflammatory properties Third Report of the NCEP Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III). Circulation. 2002;106:3143-3421.
Meta-Analysis: Predictive Value of HDL-C • Coronary Primary Prevention Trial (CPPT) • Multiple Risk Factor Intervention Trial (MRFIT) • Lipid Research Clinics Prevalence Mortality Follow-up Study (LRCS) • Framingham Heart Study (FHS) 1 mg/dL Increase in HDL-C CPPT MRFIT LRCS LRCS FHS FHS 2%CHDRisk in Men 3% CHD Risk in Women Gordon DJ, et al. Circulation. 1989;79:8-15.
Statin Treatment Does Not Eliminate Vascular Risk Associated With Low HDL-C CTT Meta-Analysis of 14 Statin Trials Control (n = 45 002) Treatmentb (n = 45 054) 5-Year Risk of Major Vascular Eventsa, % ≤35 35-42.5 >42.5 HDL-C, mg/dL aCombined outcome of nonfatal MI, CHD death, nonfatal or fatal stroke, or coronary revascularization bEvent rate per 1 mmol/L (39 mg/dL) reduction in LDL-C Baigent C, et al. Lancet.2005;366;1267-1278.
Low HDL-C Increases CVD Risk Even if LDL-C Levels Are Well-Controlled Treating to New Targets (TNT) Study Patients With LDL-C ≤70 mg/dL on Statina,b 5-Year Risk of Major CVD Events, % Q1 <37 Q2 37 to <42 Q3 42 to <47 Q4 47 to <55 Q5 ≥55 HDL-C Quintiles,a mg/dL Hazard Ratio Versus Q1* 0.85 0.57 0.55 0.61 aOn-treatment level (3 months statin therapy); n = 2661 bMean LDL-C, 58 mg/dL; mean TG, 126 mg/dL *P=.03 for differences among quintiles of HDL-C Barter P, et al. New Engl J Med. 2007;357:1301-1310.
Potential Antiatherogenic Actions of HDL VasodilatoryActivity Anti-inflammatory Activity Antithrombotic Activity HDL Antiapoptotic Activity Reverse Cholesterol Transport CellularCholesterolEfflux Anti-infectious Activity Antioxidative Activity EndothelialRepair Apo A-I Apo A-II Chapman MJ, et al. Curr Med Res Opin. 2004;20:1253-1268. Assmann G, et al. Annu Rev Med. 2003;53:321-341.
Triglyceride Level Is Significant CVD Risk Factor Recent Meta-Analysis of 29 Studies N = 262 525 Groups CHD Cases CHD Risk Ratioa (95% CI) Duration of follow-up ≥10 years 5902 <10 years 4256 Sex Male 7728 Female 1994 Fasting status Fasting 7484 Nonfasting 2674 Adjusted for HDL Yes 4469 No 5689 Overall CHD Risk Ratioa 1.72 (1.56-1.90) Decreased Risk Increased Risk 1 2 aIndividuals in top versus bottom third of usual log-triglyceride values, adjusted for at least age, sex, smoking status, lipid concentrations, and blood pressure (most) Sarwar N, et al. Circulation. 2007;115:450-458.
TG >150 mg/dL Increases CHD Eventsa in Patients With ACS on Statinsb PROVE IT-TIMI 22 Trial N = 4162 LDL-C TG 0.20 HR: 0.81 (0.68, 0.96) P=.015 HR: 0.73 (0.62, 0.87) P<.001 0.20 TG ≥150 LDL-C ≥70 0.15 0.15 CHD Eventa Rate, % CHD Eventa Rate, % 0.10 0.10 LDL-C <70 TG <150 0.05 0.05 0.00 0.00 0 150 330 510 700 0 150 330 510 700 Days After Month 1 Visit Days After Month 1 Visit Each 10 mg/dL in TG = 1.8% in CHD risk (P<.001) ACS, acute coronary syndrome aDeath, MI, and recurrent ACS bAtorvastatin 80 mg or pravastatin 40 mg Lipid values are in mg/dL Miller M, et al. J Am Coll Cardiol. 2008;51:724-730.
TG <150 mg/dL Associated With Lower Risk of CHD Eventsa Independent of LDL-C Level PROVE IT-TIMI 22 Trialb N = 4162 • Achieving both low LDL-C and low TG (<150 mg/dL) may be important therapeutic strategies in patients after an ACS Referent HR: 0.85 P=.180 CHD Eventa Rate After 30 Daysc, % HR: 0.84 P=.192 HR: 0.72 P=.017 LDL-C ≥70 LDL-C <70 TG <150 TG ≥150 aDeath, MI, and recurrent ACS bACS patients on atorvastatin 80 mg or pravastatin 40 mg cAdjusted for age, gender, low HDL-C, smoking, hypertension, obesity, diabetes, prior statin therapy, prior ACS, peripheral vascular disease, and treatment Lipid values are in mg/dL Miller M, et al. J Am Coll Cardiol. 2008;51:724-730.
NCEP ATP III: TG-Rich Remnant Lipoproteins Are Atherogenic • Elevated triglyceride levels are a marker for elevated levels of atherogenic remnant lipoproteins • VLDL-C is the most readily available measure of atherogenic remnant lipoproteins for clinical practice • When triglyceride levels are elevated, non–HDL-C (LDL-C + VLDL-C) better represents the concentrations of all atherogenic lipoproteins than LDL-C alone • Non–HDL-C should be a secondary target of therapy when triglyceride levels are ≥200 mg/dL Third Report of the NCEP Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III). Circulation. 2002;106:3143-3421.
NCEP ATP III: Non–HDL-C • Non–HDL-C calculation1 • Non–HDL-C = TC – HDL-C • Non–HDL-C = LDL-C + VLDL-C + IDL-C + Lp(a) • Non–HDL-C goal1 • Normal VLDL-C defined as value when TG <150 mg/dL (30 mg/dL) • Non–HDL-C goal is 30 mg/dL above goal for LDL-C 1Third Report of the NCEP Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III). Circulation. 2002;106:3143-3421.
Within non–HDL-C levels, no association was found between LDL-C and the risk for CHD In contrast, a strong positive and graded association between non–HDL-C and risk for CHD occurred within every level of LDL-C Non–HDL-C is a stronger predictor of CHD risk than LDL-C Non–HDL-C Is Superior to LDL-C in Predicting CHD Risk The Framingham Study Relative CHD Risk ≥190 160-189 <160 <130 130-159 ≥160 Non–HDL-C, mg/dL LDL-C, mg/dL Liu J, et al. Am J Cardiol. 2006;98:1363-1368.
Future CV Events in Initially Healthy Women by Baseline Lipids: WHS Ridker PM, et al. JAMA. 2005;294:326-333.
LRC Follow-Up Study: CVD Mortality by Non–HDL-C and LDL-C in Men 0 0.25 0.50 0.75 1.00 1.25 1.50 1.75 2.00 2.25 2.50 2.75 3.00 RR With 95% CI LRC = Lipid Research Clinics RR = Relative Risk CI = Confidence Interval Cui Y, et al. Arch Intern Med. 2001;161:1413-1419.
LRC Follow-Up Study: CVD Mortality by Non–HDL-C and LDL-C in Women 0 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 RR with 95% CI LRC = Lipid Research Clinics RR = Relative Risk CI = Confidence Interval Cui Y, et al. Arch Intern Med. 2001;161:1413-1419.
Relative Risk Ratios of Fatal MI by Quartiles of Apo B and Apo A-I: AMORIS Men <70 years Women <70 years Risk Ratio Risk Ratio 180 172 139 129 110 106 90 Apo B, mg/dL 80 Apo B, mg/dL Apo A-I, mg/dL Apo A-I, mg/dL Walldius G, et al. Lancet. 2001;358:2026-2033.
Summary • Residual CVD risk remains after patients are treated with statins (even intensive statin therapy) to reduce LDL-C • HDL-C is an independent risk factor for CHD and contributes to residual risk for atherosclerosis and CVD even if LDL-C is well-controlled • The combination of low HDL-C with elevated TG, LDL-C, and non–HDL-C is particularly atherogenic • HDL may have several antiatherogenic actions, including its role in promoting reverse cholesterol transport
Patients With CHD Risk EquivalentsaNot Achieving Potential Lipid Goals CHD (n = 635) CHD Risk Equivalenta (n = 877) Patients Not Achieving Goal, % LDL-C <100 mg/dL HDL-C ≥40 mg/dL(men) ≥50 mg/dL (women) Non–HDL-Cb <130 mg/dL ≥1 Lipid Goal a96% had diabetes bIn patients with TG ≥200 mg/dL Alsheikh-Ali AA, et al. Am J Cardiol. 2006;98:1231-1233.
Patients With CHD Risk Equivalentsa and Low HDL-C or High TG Taking Niacin or Fibrates Niacin Fibrates Niacin + Fibrates Patients, % Low HDL-C n = 577 Elevated TGb n = 158 a96% had diabetes bTG ≥200 mg/dL Alsheikh-Ali AA, et al. Am J Cardiol. 2006;98:1231-1233.
National Guideline Recommendations for Treating Beyond LDL-C
Treating Beyond LDL-C:Other Targets of Lipid-Lowering Therapy • Lipoprotein species other than LDL are involved in atherogenesis (ie, VLDL, IDL, HDL)1 • NCEP ATP III concluded that elevated non–HDL-C in patients with hypertriglyceridemia will impart increased risk even after the goal of LDL-C has been reached1 • Non–HDL-C should be a secondary target of therapy when triglyceride levels are ≥200 mg/dL2 • NCEP ATP III 2004 update: “For those high risk patients who have elevated triglycerides or low HDL-C levels, addition of a fibrate or nicotinic acid to LDL-lowering therapy can be considered.”3 1Grundy SM. Circulation. 2002;106:2526-2529. 2Third Report of the NCEP Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III). Circulation. 2002;106:3143-3421. 3Grundy SM, et al. Circulation. 2004;110:227-239.
American Diabetes Association (ADA)Standards of Medical Care in Diabetes:Dyslipidemia Management a<70 mg/dL is an option in patients with overt CVD b Niacin may increase blood glucose at high doses American Diabetes Association. Diabetes Care. 2008;31(suppl 1):S12-S54. American Diabetes Association. Diabetes Care. 2004;27:S68-S71.
National Guideline Recommendations for Treating Beyond LDL-C: Combination Therapy ADA/AHA 2007 Scientific Statement1 Primary Prevention of CVD in Patients With Diabetes • “Combination therapy of LDL-lowering drugs (eg, statins) with fibrates or niacin may be necessary to achieve lipid targets…” AHA/ACC 2006 Guideline Update2 Secondary Prevention for Patients With CVD • Therapeutic options to reduce non–HDL-C (<130 mg/dLa) are • More intense LDL-C–lowering therapy • Add niacin (after LDL-C–lowering therapy) • Add fibrate (after LDL-C–lowering therapy) 1Buse JB, et al. Diabetes Care. 2007;30:162-172. 2Smith SC, et al. Circulation. 2006;113:2363-2372. aFurther reduction of non–HDL-C to <100 mg/dL is reasonable
ADA/ACC 2008 Consensus Statement:Treatment Goals in Patients With Cardiometabolic Risk and Lipoprotein Abnormalities “In individuals on statin therapy who continue to have low HDL-C or elevated non–HDL-C, especially if Apo B levels remain elevated,combination therapy is recommended. The preferred agent to use in combination with a statin is nicotinic acid…” aMajor risk factors beyond dyslipidemia include smoking, hypertension, and family history of premature CHD Brunzell JD, et al. Diabetes Care. 2008;31:811-822.
Agents That Raise HDL-C AgentHDL-C ↑Primary Use Nicotinic acid 15-35% ↑ HDL Fibrates 5-20% ↓ TG Statins 5-15% ↓ LDL Rx omega-3a 5-10% ↓ TG Bile-acid resinsa 2-5% ↓ LDL Ezetimibea 1-3% ↓ LDL Pioglitazonea5-20% ↓ Glucose Estrogensa 10-25% ↓ Hot flashes -blockersa10-20% ↓ BPH Alcohola5-10% Social aWithout FDA-approved indication for HDL-raising Adapted from Belalcazar LM, et al. Prog Cardiovasc Dis. 1998;41:151-174. Insull W, et al. Mayo Clin Proc. 2001;76:971-982. McKenney JM, et al. Pharmacotherapy. 2007;27:715-728.
Clinical Trial Evidence Supporting Treating Beyond LDL-C to Reduce CVD Risk
Coronary Drug Project: Macrovascular Outcomesa 15% Reduction P<.05 Placebo (n = 2789) Niacin (n = 1119) 26% Reduction P<.05 24% Reduction P<.05 Event Rate, % 47% Reduction P<.05 CHD Death/ Nonfatal MI Nonfatal MI Stroke/TIA CV Surgeryb aTotal follow-up experience (mean, 6.2 yrs) b5-year incidence TIA, transient ischemic attack CDP Research Group. JAMA. 1975;231:360-381.
CDP: Reduction in Recurrence of MIa by Baseline Fasting Plasma Glucose Placebo (n = 2787) Niacin 3000 mg (n = 1119) Interactive P-value = NS 57% Reduction 30% Reduction 25% Reduction 24% Reduction Nonfatal MI Event Rate, % <95 95-104 105-125 ≥126b Baseline Fasting Plasma Glucose, mg/dL a6-year follow-up bADA definition of diabetes Canner PL, et al. Am J Cardiol. 2005;95:254-257.
CDP: 15-Year Follow-Up Placebo (n = 2008) 11% Reduction P=.0004 Niacina (n = 827) 12% Reduction P<.05 Event Rate, % Total Mortality CHD Mortality Canner PL, et al. J Am Coll Cardiol. 1986;8:1245-1255. aPatients had not received niacin for ~9 years
HHS: Marked Reduction of CHD Events in Patients With High Triglyceride Levels and LDL/HDL Ratio 30 Placebo Gemfibrozil 25 71% Reduction P<.005 20 per 1000 Person-Years Incidence of Cardiac Events 15 10 5 0 TG >204 TG >204 TG ≤204 TG ≤204 LDL/HDL ≤5 LDL/HDL >5 Triglyceride values are in mg/dL. Manninen V, et al. Circulation. 1992;85:37-45.
VA-HIT: Treating Dyslipidemia Beyond LDL-C Improves Clinical Outcomes % Change (Gemfibrozil Versus Placebo) † LDL-C HDL-C TG Nonfatal CHD Strokea MI or CHD Death VA-HIT = Veterans Affairs High-Density Lipoprotein Intervention Trial 2531 men with CHD, HDL-C ≤40 mg/dL, and LDL-C ≤140 mg/dL were randomized to gemfibrozil (1200 mg/d) or placebo and followed for a median of 5.1 years *P0.05; †P=0.07;aInvestigator-designated Rubins HB, et al. N Engl J Med. 1999;341:410-418.
FIELD: Primary and Secondary End Points 11% Reduction P=.035 Placebo Fenofibrate 21% Reduction P=.003 11% Reduction P=.16 24% Reduction P=.01 19% Increase P=.22 CHD Eventsa (Primary EP) Nonfatal MI CHD Death Total CVD Eventsb (Secondary EP) Coronary Revascularization aNonfatal MI and CHD death bCHD events, stroke, CVD death, revascularizations Keech A, et al. Lancet. 2005;366:1849-1861.
FIELD: Fenofibrate Reduces the Risk for Vascular Complications of Diabetes Macrovascular Microvascular CVD Angina Risk Reduction, % Nonfatal MI Albuminuria Amputations Coronary Revasc. Retinal Laser Therapy P=.01 P=.035 P=.003 P=.04 P=.011 P=.0003 P=.002 Keech A, et al. Lancet. 2005;366(9500):1849-1861. Keech A. Atherosclerosis Supplements. 2006;7:342. Abstract.
FIELD: Rapid Onset of Retinal Benefits Within 8 Months of Treatment Allocation First Laser Treatment for Diabetic Retinopathy 6.0 Placebo 5.0 4.0 Cumulative Risk, % Fenofibrate 3.0 2.0 HR 0.69; P=.0002 1.0 0 0 1 2 3 4 5 6 Years After Randomization Number At Risk Placebo 4900 4784 4674 4559 4485 2524 837 Fenofibrate 4895 4797 4706 4626 4515 2540 845 Keech A, et al. Lancet. 2007;370:1687-1697.
Low-Dose Prescription Omega-3 Fatty Acids Reduce CVD After Myocardial Infarction GISSI-P Results Control (n = 2828) Omega-3 FA 1 g (n = 2836) 15% Reduction P=.023 20% Reduction P=.008 Event Rate, % Death/ Nonfatal MI/ Nonfatal Stroke CVD Death/ Nonfatal MI/ Nonfatal Stroke GISSI-P Investigators. Lancet. 1999;354(9177):447-455.
Effect of Combination Lipid-Modifying Therapy on Atherosclerosis and CVD
Simultaneous LDL-C Lowering and HDL-C Elevation for Optimal CVD Reduction Meta-Analysis of 23 Lipid Trials • The cardiovascular event rate reductions associated with a decrease in LDL-C and an increase in HDL-C are statistically independent • Meta-analysis revealed that the sum of % increase in HDL-C and % decrease in LDL-C (%HDL + %LDL)predicts cardiovascular benefits more effectively than either component alone • This analysis supports the notion that a readily attainable 40% reduction in LDL-C combined with a 30% elevation in HDL-C will result in ~70% CHD risk reduction and a revolution in cardiovascular prevention N = 83 000 Brown BG, et al. Curr Opin Lipidol. 2006;17:631-636.
Simultaneous LDL-C Lowering and HDL-C Elevation for Optimal CVD Reduction Meta-Analysis of 23 Lipid Trials: QCA 4 Placebo (6) 3 2 Fibrates (1) Change From Baseline in Mean Proximal Percent Stenosis, %S Statins (6) 1 Progression 0 Niacin combos (4) Regression Statin + resin (1) -1 -2 0 25 50 75 %HDL-C - %LDL-Ca aPlacebo-adjusted Brown BG, et al. Curr Opin Lipidol. 2006;17:631-636.
Simultaneous LDL-C Lowering and HDL-C Elevation for Optimal CVD Reduction Meta-Analysis of 23 Lipid Trials: CVD Events Placebo (23) 0 -20 Fibrates (3) Statins (11) Niacin (1) Ileal bypass (1) Reduction in CVD Event Rate Versus Placebo, % -40 Niacin combos (5) -60 Statin + resin (1) -80 0 25 50 75 %HDL-C - %LDL-Ca aPlacebo-adjusted Brown BG, et al. Curr Opin Lipidol. 2006;17:631-636.
Familial Atherosclerosis Treatment Study (FATS): Angiographic Results (QCA)a Progression of coronary lesion Regression of coronary lesion * * Patients, % Conventional Therapy Colestipol + Lovastatin Colestipol + Niacin N = 120 men with CAD a2.5 year follow-up *P<.005 versus conventional therapy Brown G, et al. N Engl J Med. 1990;323:1289-1298.