Download
1 / 23
260 likes | 440 Views
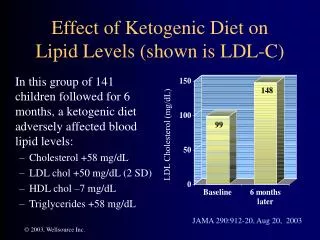
Learn about the significance of LDL-P and LDL-C, how they impact cardiovascular disease risk, and why measuring LDL particle number is crucial for accurate risk assessment. Discover key findings from studies like the Framingham Offspring Study and Multi-Ethnic Study of Atherosclerosis.

E N D
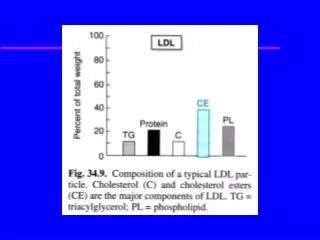
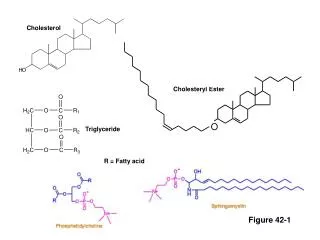
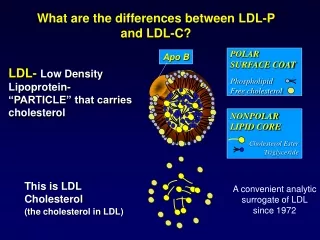
POLAR SURFACE COAT Phospholipid Free cholesterol Apo B NONPOLAR LIPID CORE Cholesterol Ester Triglyceride This is LDL Cholesterol (the cholesterol in LDL) What are the differences between LDL-P and LDL-C? LDL- Low Density Lipoprotein- “PARTICLE” that carries cholesterol A convenient analytic surrogate of LDL since 1972
VLDL Chylomicron Remnants LDL Cholesterol Triglycerides (mainly) HDL2 HDL Cholesterol HDL3 What are various types of Lipoproteins? 0.95 IDL 1.006 Decreasing Density / Density (g/ml) 1.02 LDL 1.06 1.10 1.20 5 10 20 40 60 80 1000 Increasing Size /Diameter (nm)
Gradient driven process…LDL Particles invade the arterial wall So Why Is LDL So Important in CVD? The higher the number of LDL particles (LDL-P), the greater the risk for CHD. • Oxidative Modification • Foam Cell Formation • Atherosclerosis 2 Fredrickson et al. NEJM 1967; 276: 148
Cholesterol Is an Inadequate Predictor of Risk • Framingham Heart Study Indicates that Measuring Cholesterol Does Not Tell Us Enough • 80% of people who had an MI had similar cholesterol levels as those who did not have an MI • 50% of people who suffered a heart attack had normal cholesterol levels • Women, patients with diabetes or metabolic syndrome, and family history are “enriched” populations
Up to 70% More Particles 100 mg/dL 100 mg/dL Large LDL Small LDL Cholesterol Balance Small LDL Particles Contain Less Cholesterol Than Large LDL Particles • With the same LDL cholesterol level, a person with small LDL has more particles and a higher disease risk than someone with large LDL due to an increased number of LDL particles (LDL-P).
Global Metabolic Risk (CMR) is a multitude of risk factors which occur together or separately that increase risk for Type II DM and CVD. • Many patients with CMR or diabetes have relatively normal levels of LDL cholesterol (LDL-C) but may have increased LDL particle numbers (LDL-P) • Even with adequate LDL-C lowering, many patients on statin therapy still have significant residual CVD risk. Brunzell et.al.,JACC.2008;51:1513
Key Findings in ADA / ACC Consensus Statement • “Even with adequate LDL Cholesterol lowering, many patients on statin therapy have significant residual CVD risk.” • “ApoB and LDL particle number are more discriminating measures of the adequacy of LDL lowering therapy than are cholesterol or non-HDL cholesterol.” • “ApoB and LDL particle concentration also appear to be more closely associated with obesity, diabetes, insulin resistance, and other markers of CMR than LDL cholesterol or non-HDL cholesterol.” • “Many cross-sectional and prospective studies show that LDL particle number is a better discriminator of risk than is LDL cholesterol.”
Outcome Associations of NMR LDL Particle Number (LDL-P) versus LDL Cholesterol (LDL-C) * Significant and independent after multivariate modeling (lipids and established risk factors)
Framingham Offspring Study • Long-running NIH/NHLBI observational study of residents of Framingham, MA to determine risk factors for future cardiovascular disease (CVD). • Blood samples were obtained in 1988-91 (exam 4). Lipoprotein particles were measured by NMR spectroscopy (LipoScience) and lipids by traditional chemical methods. • CVD occurrence was monitored during 15-year follow-up. There were 431 CVD events (MI, stroke, CHD death, angina, congestive heart failure) among 3,066 subjects. Publications to date: Freedman DS et al., Clin Chem 2004;50:1189-1200. Kathiresan S et al., Circulation 2006;113:20-29. Cromwell W et al., J Clin Lipidol 2007;1:57-64.
Event-Free Survival Years of Follow-up Concordant LDL-C and LDL-P in Framingham ( Cromwell et al. J Clin Lipidol 2007;1:583-92) Better survival Lower risk Low LDL-C Low LDL-P (n=1,249) Worse survival Higher risk High LDL-C High LDL-P (n=1,251) Median LDL-P= 1414 nmol/L, Median LDL-C 131 mg/dL
Event-Free Survival Years of Follow-up Discordant LDL-C and LDL-P in Framingham ( Cromwell et al. J Clin Lipidol 2007;1:583-92) Better survival Lower risk High LDL-C Low LDL-P (n=284) Worse survival Higher risk Low LDL-C High LDL-P (n=282) Median LDL-P= 1414 nmol/L, Median LDL-C 131 mg/dL
LDL-C LDL-P Alternate LDL Measures in Framingham Men with Increasing Numbers of Metabolic Syndrome Features 0 1 2 3 4 5 N=286 N=407 N=355 N=233 N=113 N=30 MetSyn (+) MetSyn (-) ~2.3x risk Kathiresan S, et al. Circulation 2006;113:20-27
LDL-C LDL-P Alternate LDL Measures in Framingham Women with Increasing Numbers of Metabolic Syndrome Features 0 1 2 3 4 5 N=562 N=464 N=298 N=134 N=102 N=29 MetSyn (+) MetSyn (-) ~2.3x risk Kathiresan S, et al. Circulation 2006;113:20-27
Multi-Ethnic Study of Atherosclerosis (MESA) • MESA is a large (n=6,814) multi-center NIH/NHLBI observational study of the pathogenesis and progression of subclinical atherosclerosis. • Mean age 61.4 years • Study population- 38% White, 28% African American, 22% Hispanic, and 12% Chinese, with 53% women • Baseline blood samples permit study of relations of lipids and lipoproteins to carotid atherosclerosis (intima-media thickness, IMT), and shortly also to incident CVD events. • Lipoprotein particle measurements were performed by nuclear magnetic resonance (NMR) spectroscopy at LipoScience (Raleigh, NC) Publications to date: Mora S et al., Atherosclerosis 2007;192:211-217.
Discordant LDL-P >LDL-C by +20 percentile 922 (17%) 1799 Cholesterol-poor 104 1509 Concordant < 20 percentile difference 3,498 (65%) 2368 119 1320 Discordant LDL-P < LDL-C by -20 percentile 942 (18%) 3167 Cholesterol-rich 136 1128 Concordance/Discordance Between LDL-C and LDL-P in MESA N (%) Cholesterol Molecules per LDL Particle LDL-C (mg/dL) LDL-P (nmol/L) J. Otvos, unpublished data
Overall 5,362 39.9 (p<0.0001) 35.8 (p<0.0001) Discordant ±10 percentile 3,235 (60%) 37.7 (p<0.0001) 22.7 (p=0.0003) Discordant ±20 percentile 1,864 (35%) 37.6 (p<0.0001) 13.4 (p=0.13) Discordant ±30 percentile 978 (18%) 40.2 (p=0.0011) 3.1 (p=0.79) Relations of LDL-P and LDL-C with Carotid Atherosclerosis in MESA N (%) IMT in µm per 1 SD LDL-P IMT in µm per 1 SD LDL-C Data are from multiple linear regression models adjusted for age, gender, race, hypertension, and smoking. Analysis is restricted to subjects not taking lipid altering medications. LipoScience, unpublished data
Relations of Non-HDLc and LDLp with Carotid IMT in Concordant and Discordant MESA Subgroups 1 Non-HDLc and LDLp values differ by < ±20 percentile units 2 Non-HDLc and LDLp values differ by ±20 percentile units
A prospective comparison of nuclear magnetic resonance lipoprotein profiles in predicting incident diabetes in 26,911 initially healthy women Samia Mora, James Otvos, Aruna Pradhan, Julie E. Buring, Paul M RidkerBrigham and Women’s Hospital, Boston, MA ACC Meeting, April 1 2008
Objective To compare NMR-measured lipoprotein profiles with chemically-measured standard lipids in predicting clinical diagnosis of DM2
Methods: Study Design • Prospective study of apparently healthy women (Women’s Health Study) • N=26,911 (after excluding baseline DM2, N=762) • Follow-up: 10.9 ± 1.6 y • Main outcome measure: Incident clinical diagnosis of DM2; N=1,156
LDL Measures *Adjusted for age, smk, ASA/VE assignment, menopause, HRT, BP, BMI
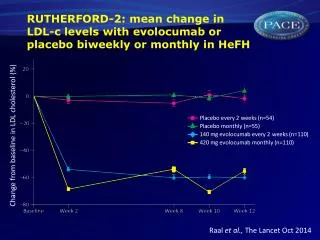
Effects of LDL-lowering therapy on LDL-C and LDL-P Sniderman. J Clin Lipidol 2008;2:36-42